

Risk-Adapted Postmastectomy Radiotherapy Decision Based on Prognostic Nomogram for pT1-2N1M0 Breast Cancer: A Multicenter Study
- PMID: 33363018
- PMCID: PMC7761288
- DOI: 10.3389/fonc.2020.588859
Risk-Adapted Postmastectomy Radiotherapy Decision Based on Prognostic Nomogram for pT1-2N1M0 Breast Cancer: A Multicenter Study
Abstract
Purpose: The aim of this study was to develop a widely accepted prognostic nomogram and establish a risk-adapted PMRT strategy based on locoregional recurrence for pT1-2N1M0 breast cancer.
Methods and materials: A total of 3,033 patients with pT1-2N1M0 breast cancer treated at 6 participating institutions between 2000 and 2016 were retrospectively reviewed. A nomogram was developed to predicted locoregional recurrence-free survival (LRFS). A propensity score-matched (PSM) analyses was performed in risk-adapted model.
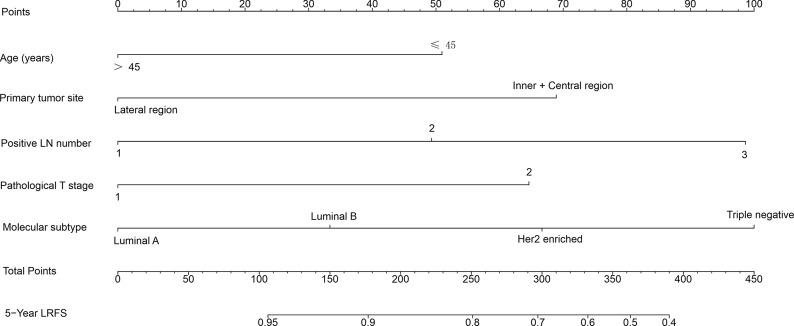
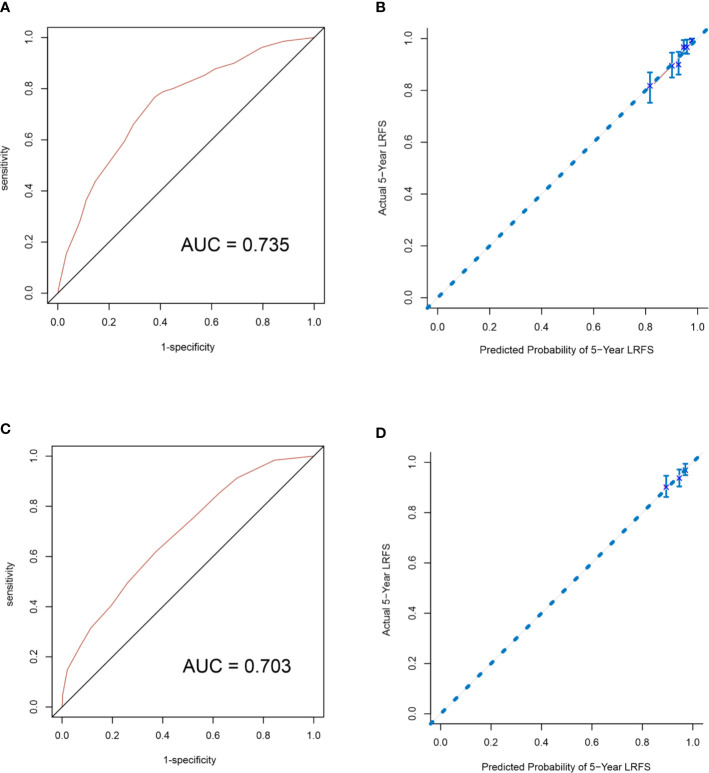
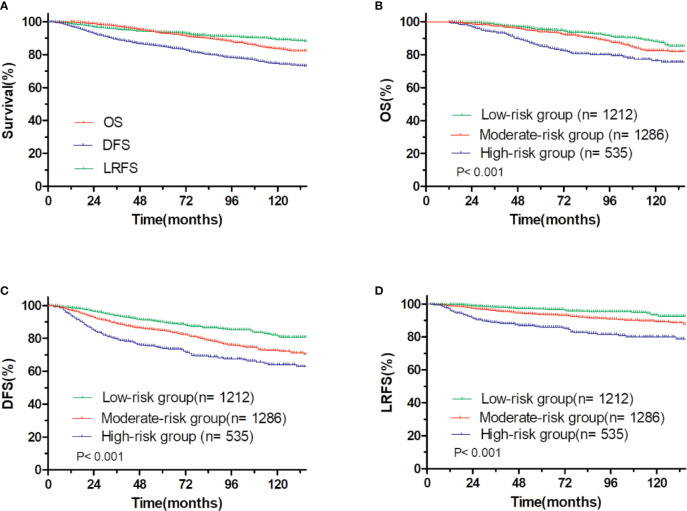
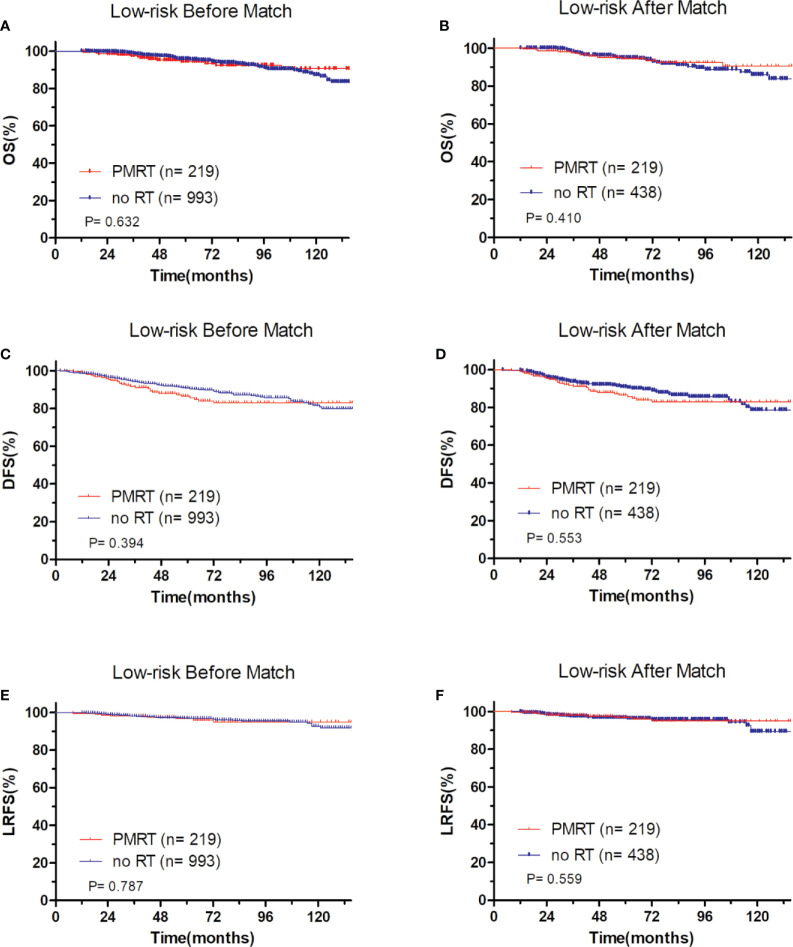
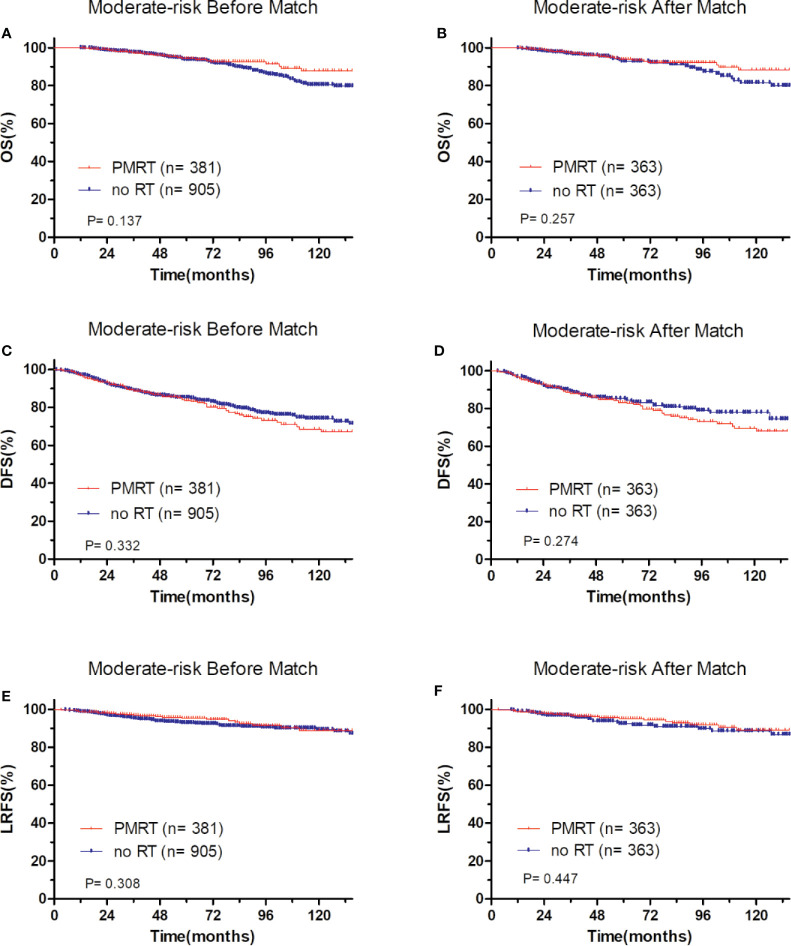
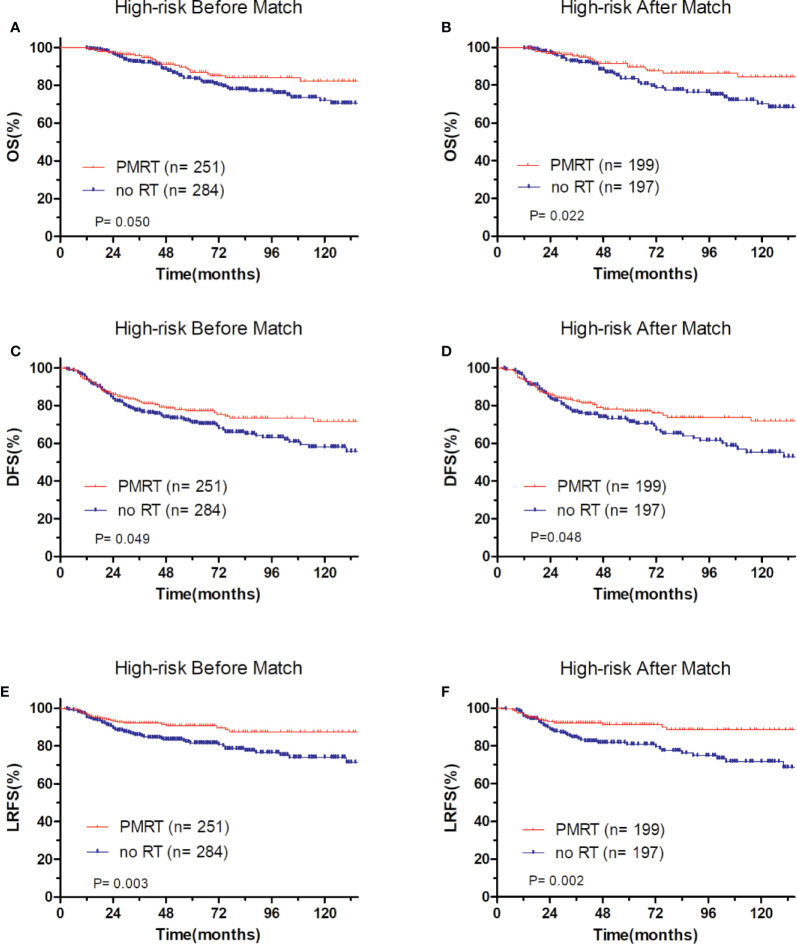
Results: With the median follow-up of 65.0 months, the 5-year overall survival (OS), disease free survival (DFS) and LRFS were 93.0, 84.8, and 93.6%, respectively. There was no significant difference between patients who received PMRT or not for the entire group. A nomogram was developed and validated to estimate the probability of 5-year LRFS based on five independent factors including age, primary tumor site, positive lymph nodes number, pathological T stage, and molecular subtype that were selected by a multivariate analysis of patients who did not receive PMRT in the primary cohort. According to the total nomogram risk scores, the entire patients were classified into low- (40.0%), moderate- (42.4%), and high-risk group (17.6%). The 5-year outcomes were significantly different among these three groups (P<0.001). In low-risk group, patients who received PMRT or not both achieved a favorable OS, DFS, and LRFS. In moderate-risk group, no differences in OS, DFS, and LRFS were observed between PMRT and no PMRT patients. In high-risk group, compared with no PMRT, PMRT resulted in significantly different OS (86.8 vs 83.9%, P = 0.050), DFS (77.2 vs 70.9%, P = 0.049), and LRFS (90.8 vs. 81.6%, P = 0.003). After PSM adjustment, there were no significant differences in OS, DFS, and LRFS in low-risk and moderate-risk groups. However, in the high-risk group, PMRT still resulted in significantly better OS, DFS and improved LRFS.
Conclusions: The proposed nomogram provides an individualized risk estimate of LRFS in patients with pT1-2N1M0 breast cancer. Risk-adapted PMRT for high-risk patients is a viable effective strategy.
Keywords: breast neoplasms; mastectomy; molecular subtype; nomogram; prognosis; radiation therapy; recurrence; risk-adapted therapy.
Copyright © 2020 Li, Yue, Wan, Hua, Yang, Yang, Zhang, Pei, Han, Xu and Xia.
Conflict of interest statement
Authors YX and XX were employed by company Geneplus-Beijing Institute. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
[Risk-adapted postmastectomy radiotherapy based on local-regional recurrence for T1-2N1M0 breast Cancer].Zhonghua Zhong Liu Za Zhi. 2017 Nov 23;39(11):841-849. doi: 10.3760/cma.j.issn.0253-3766.2017.11.007. Zhonghua Zhong Liu Za Zhi. 2017. PMID: 29151291 Chinese.
-
The significance of risk stratification through nomogram-based assessment in determining postmastectomy radiotherapy for patients diagnosed with pT1 - 2N1M0 breast cancer.Radiat Oncol. 2024 Sep 13;19(1):120. doi: 10.1186/s13014-024-02510-w. Radiat Oncol. 2024. PMID: 39272162 Free PMC article.
-
Postmastectomy radiotherapy improves disease-free survival of high risk of locoregional recurrence breast cancer patients with T1-2 and 1 to 3 positive nodes.PLoS One. 2015 Mar 17;10(3):e0119105. doi: 10.1371/journal.pone.0119105. eCollection 2015. PLoS One. 2015. PMID: 25781605 Free PMC article.
-
The prognostic differences and the effect of postmastectomy radiotherapy between post-chemotherapy ypT1-2ypN1 and de novo pT1-2N1 breast cancer.Cancer Med. 2023 Apr;12(7):8112-8121. doi: 10.1002/cam4.5610. Epub 2023 Feb 3. Cancer Med. 2023. PMID: 36734308 Free PMC article.
-
Does Post-Mastectomy Radiotherapy Confer Survival Benefits on Patients With 1-3 Clinically Positive Lymph Nodes Rendered Pathologically Negative After Neoadjuvant Systemic Chemotherapy: Consensus from A Pooled Analysis?Eur J Breast Health. 2024 Apr 1;20(2):81-88. doi: 10.4274/ejbh.galenos.2024.2023-12-14. eCollection 2024 Apr. Eur J Breast Health. 2024. PMID: 38571693 Free PMC article.
Cited by
-
Development and validation of nomograms for predicting survival outcomes in patients with T1-2N1 breast cancer to identify those who could not benefit from postmastectomy radiotherapy.Front Oncol. 2023 Mar 28;13:1112687. doi: 10.3389/fonc.2023.1112687. eCollection 2023. Front Oncol. 2023. PMID: 37056328 Free PMC article.
References
-
- Wallgren A, Bonetti M, Gelber RD, Goldhirsch A, Castiglione-Gertsch M, Holmberg SB, et al. Risk factors for locoregional recurrence among breast cancer patients: Results from International Breast Cancer Study Group Trials I Through VII. J Clin Oncol (2003) 21:1205–13. 10.1200/JCO.2003.03.130 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous