

Complications Following Primary Repair of Non-proximal Hypospadias in Children: A Systematic Review and Meta-Analysis
- PMID: 33363061
- PMCID: PMC7756017
- DOI: 10.3389/fped.2020.579364
Complications Following Primary Repair of Non-proximal Hypospadias in Children: A Systematic Review and Meta-Analysis
Abstract
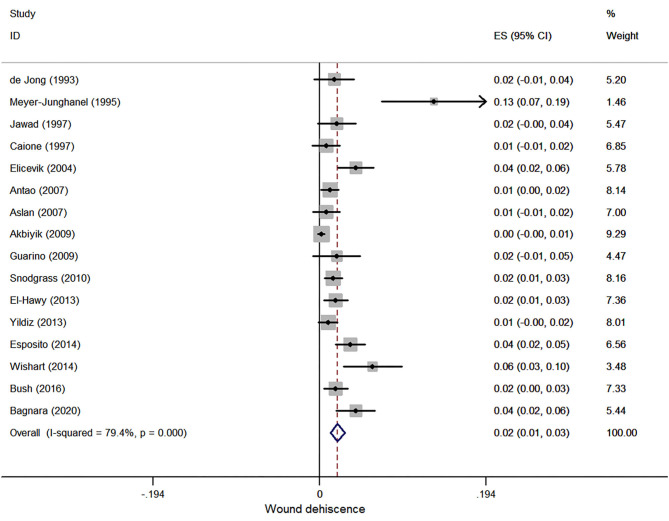
Purpose: The aim of this study was to systematically review the literature on the complications and postoperative outcomes of children with non-proximal hypospadias. Methods: Electronic databases including PubMed, Embase, and Cochrane Library CENTRAL were searched systematically from January 1990 to June 2020 for the literature that reported the postoperative outcomes of patients with non-proximal hypospadias. Non-proximal hypospadias encompassed distal and mid-penile hypospadias. Results: We included 44 studies involving 10,666 subjects. Urethrocutaneous fistula (UCF) was the most common complication with an incidence of 4.0% (95% CI, 3.1-5.0%). Incidence of overall complications was 8.0% (95% CI, 6.3-9.8%). Meta-regression analysis revealed that length of urethral stent indwelling (coefficient 0.006; 95% CI, 0.000-0.011; p = 0.036) and penile dressing (coefficient 0.010; 95% CI, 0.000-0.021; p = 0.048) were two risk factors for UCF. Multivariate meta-regression analysis did not identify any independent risk factors for UCF. No differences were found between stent and stentless groups in non-proximal hypospadias regarding incidences of UCF (OR, 0.589; 95% CI, 0.267-1.297), meatal stenosis (OR, 0.880; 95% CI, 0.318-2.437), and overall complications (OR, 0.695; 95% CI, 0.403-1.199). No differences were found between foreskin preservation and circumcision in terms of complications either. Conclusions: UCF is the most common complication following hypospadias repair with an incidence of 4.0%. Independent risk factors for UCF were not identified in the current research. Distal hypospadias repair without stent indwelling is not likely to compromise the postoperative outcome. Further studies should be designed to explore the differences between different surgical approaches and the potential risk factors for complications following hypospadias repair.
Keywords: children; complications; hypospadias; meta-analysis; surgery.
Copyright © 2020 Wu, Wang, Zhao, Wei, Han, Liu, Lin, Wei and Wu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures







References
Publication types
LinkOut - more resources
Full Text Sources