

Use of Venovenous Extracorporeal Membrane Oxygenation in Critically-Ill Patients With COVID-19
- PMID: 33363190
- PMCID: PMC7758460
- DOI: 10.3389/fmed.2020.614569
Use of Venovenous Extracorporeal Membrane Oxygenation in Critically-Ill Patients With COVID-19
Abstract
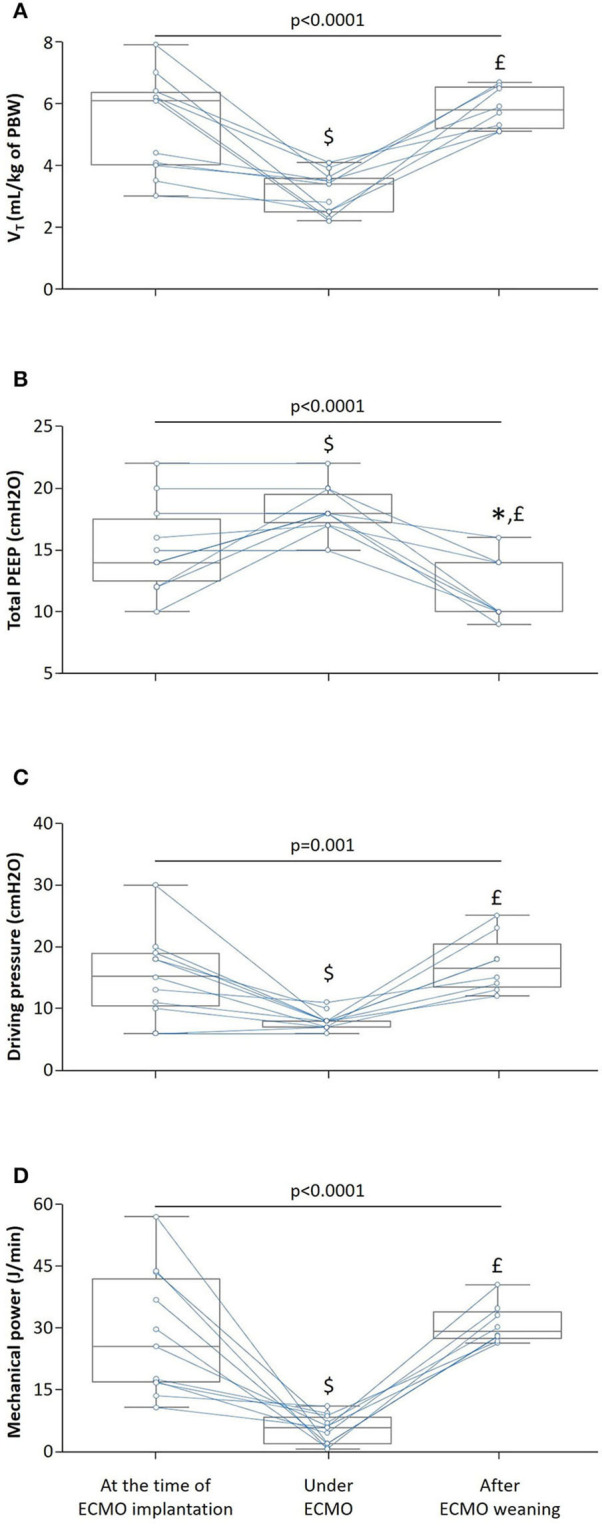
Acute respiratory distress syndrome (ARDS) related to Coronavirus disease (COVID-19) is associated with high mortality. It has been suggested that venovenous extracorporeal membrane oxygenation (ECMO) was suitable in this indication, albeit the effects of ECMO on the mechanical respiratory parameters have been scarcely described. In this case-series, we prospectively described the use of venovenous ECMO and its effects on mechanical respiratory parameters in eleven COVID-19 patients with severe ARDS. Implantation of ECMO occurred 6 [3-11] days after the onset of mechanical ventilation. At the time of ECMO implantation, all patients received neuromuscular blocking agents, three (27%) received inhaled nitric oxide and prone positioning was performed in all patients with 4 [3-5] sessions of PP per patient. Under ECMO, the tidal volume was significantly decreased from 6.1 [4.0-6.3] to 3.4 [2.5-3.6] mL/kg of predicted body weight and the positive end-expiratory pressure level was increased by 25 ± 27% whereas the driving pressure and the mechanical power decreased by 33 ± 25% and 71 ± 27%, respectively. The PaO2/FiO2 ratio significantly increased from 68 [58-89] to 168 [137-218] and the oxygenation index significantly decreased from 28 [26-35] to 13 [10-15]. The duration of ECMO was 12 [8-25] days. Nine (82%) patients experienced ECMO-related complications and the main complication was major bleeding requiring blood transfusions. Intensive care unit mortality rate was 55% but no patient died from ECMO-related complications. In COVID-19 patients with severe ARDS, venovenous ECMO allowed ultra-protective ventilation, improved oxygenation and should be considered in highly selected patients with the most severe ARDS.
Keywords: COVID-19; acute respiratory distress syndrome—ARDS; extracorporeal membrane oxygenation (ECMO); intensive care unit (ICU); mechanical ventilation.
Copyright © 2020 Jozwiak, Chiche, Charpentier, Ait Hamou, Jaubert, Benghanem, Dupland, Gavaud, Péne, Cariou, Mira and Nguyen.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Miscellaneous