

Systematic Review and Meta-analysis of COVID-19 and Kidney Transplant Recipients, the South West London Kidney Transplant Network Experience
- PMID: 33363263
- PMCID: PMC7748968
- DOI: 10.1016/j.ekir.2020.12.013
Systematic Review and Meta-analysis of COVID-19 and Kidney Transplant Recipients, the South West London Kidney Transplant Network Experience
Abstract
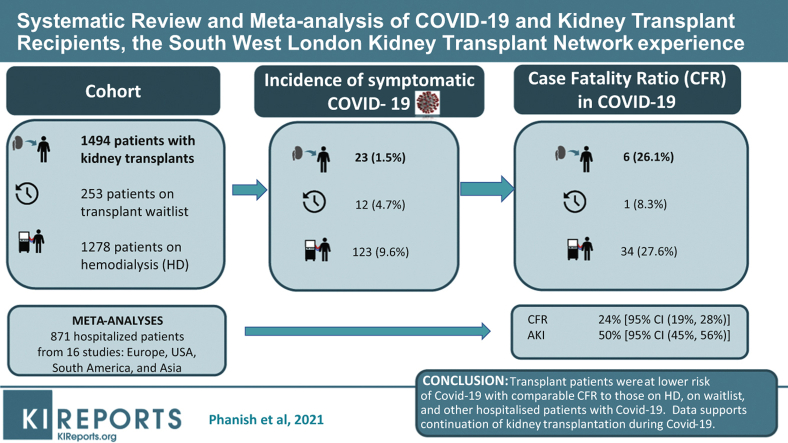
Introduction: There is paucity of literature comparing outcomes of kidney transplant patients with COVID-19 to that of dialysis and waitlisted patients. This report describes our data, provides comparative analysis, together with a meta-analysis of published studies, and describes our protocols to restart the transplant program.
Methods: Data were analyzed on kidney transplant, dialysis, and waitlisted patients tested positive for SARS-CoV-2 (nasopharyngeal swab polymerase chain reaction [PCR] test) between March 1, 2020, and June 30, 2020, together with a meta-analysis of 16 studies.
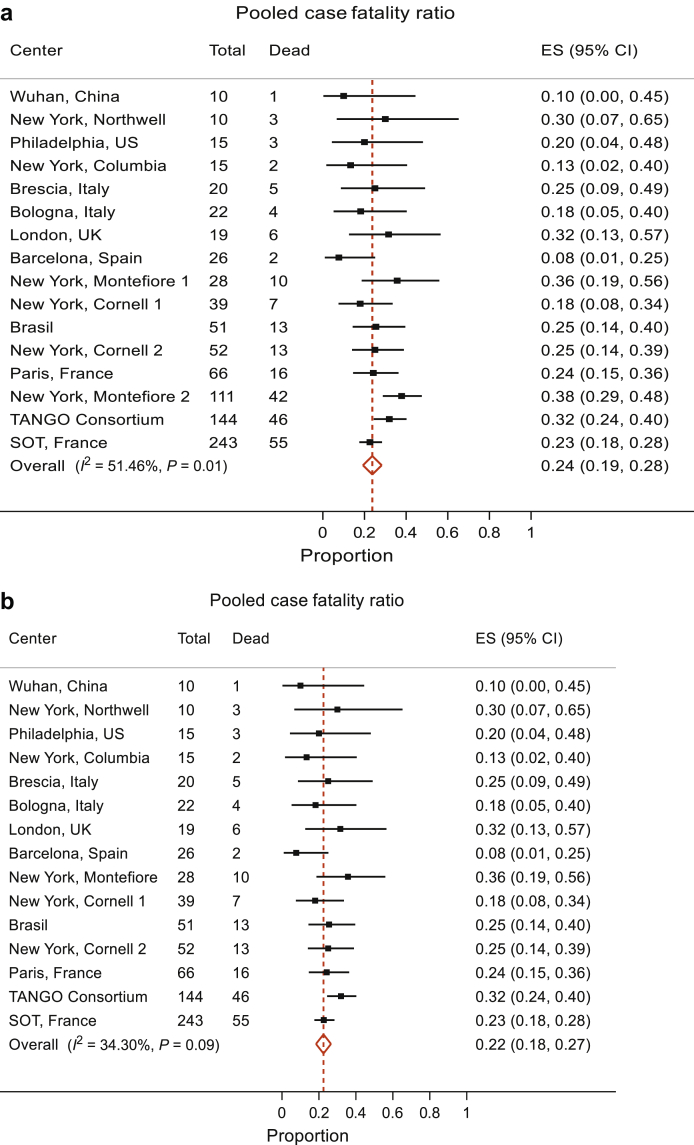
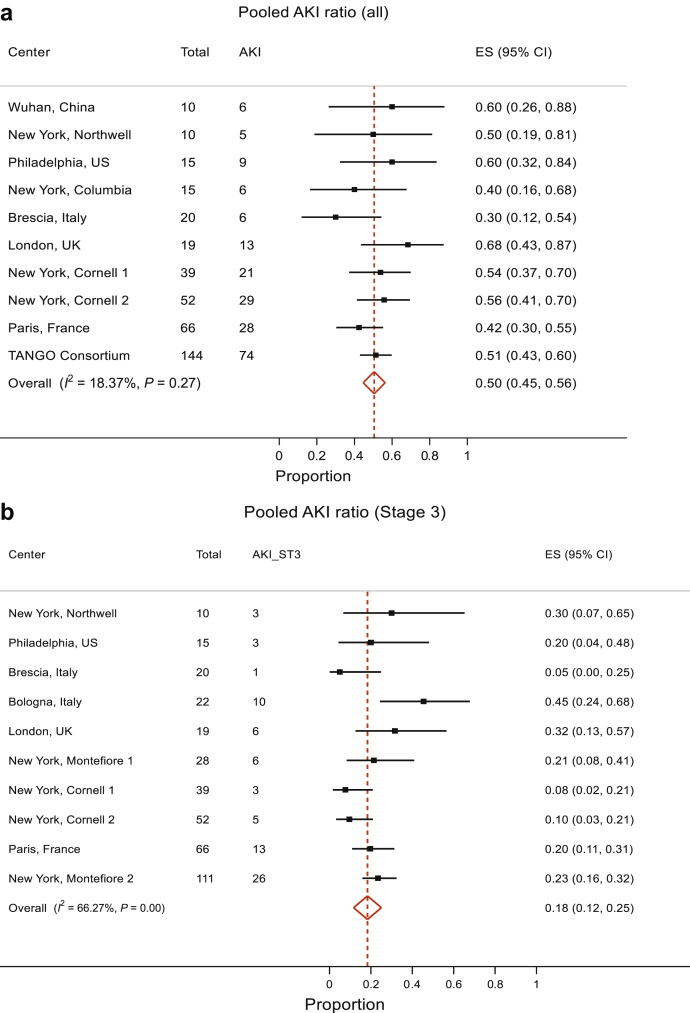
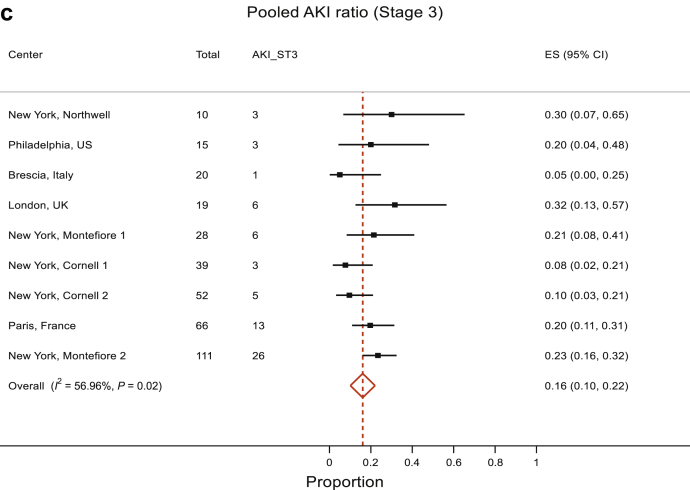
Results: Twenty-three of 1494 kidney transplant patients tested positive for SARS-CoV-2 compared with 123 of 1278 hemodialysis patients (1.5% vs. 9.6%, P < 0.001) and 12 of 253 waitlisted patients (1.5% vs. 4.7%, P = 0.002). Nineteen patients required hospital admission, of whom 6 died and 13 developed AKI. The overall case fatality ratio was 26.1% compared with patients on hemodialysis (27.6%, P = 0.99) and waitlisted patients (8.3%, P = 0.38). Within our entire cohort, 0.4% of transplant patients died compared with 0.4% of waitlisted patients and 2.7% of hemodialysis patients. Patients who died were older (alive [median age 71 years] vs. dead [median age 59 years], P = 0.01).In a meta-analysis of 16 studies, including ours, the pooled case fatality ratio was 24% (95% confidence interval [CI] 19%, 28%); AKI proportion in 10 studies was 50% (95% CI 45%, 56%), with some evidence against no heterogeneity between studies (P = 0.02).
Conclusions: From our cohort of transplant patients, a significantly lower proportion of patients contracted COVID-19 compared with waitlisted and dialysis patients. The case fatality ratio was comparable to that of the dialysis cohort and to a pooled case fatality ratio from a meta-analysis of 16 studies. The pooled AKI ratio in the meta-analysis was similar to our results.
© 2020 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
