

Clinical Relevance of the Anti-inflammatory Effects of Roflumilast on Human Bronchus: Potentiation by a Long-Acting Beta-2-Agonist
- PMID: 33363471
- PMCID: PMC7754640
- DOI: 10.3389/fphar.2020.598702
Clinical Relevance of the Anti-inflammatory Effects of Roflumilast on Human Bronchus: Potentiation by a Long-Acting Beta-2-Agonist
Abstract
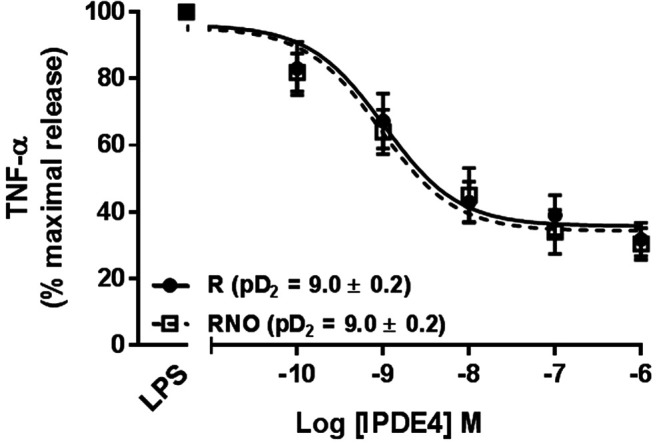
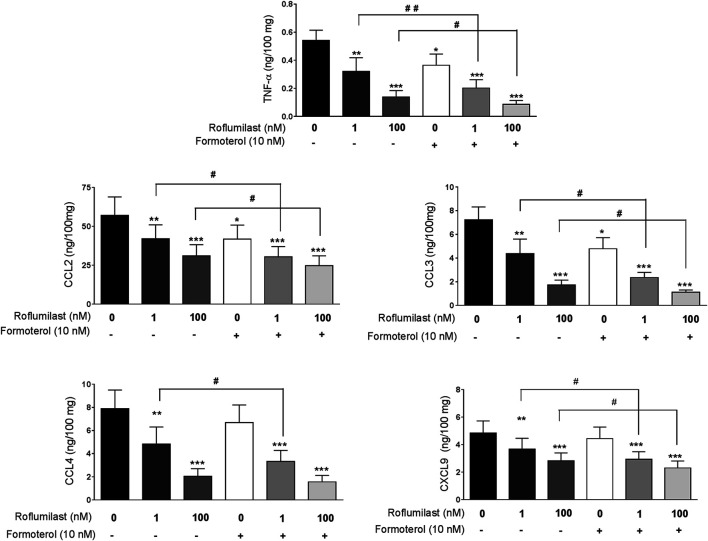
Background: Roflumilast is an option for treating patients with severe COPD and frequent exacerbations despite optimal therapy with inhaled drugs. The present study focused on whether the phosphodiesterase (PDE) 4 inhibitor roflumilast and its active metabolite roflumilast N-oxide affect the release of tumor necrosis factor (TNF)-α and chemokines by lipopolysaccharide (LPS)-stimulated human bronchial explants. We also investigated the interactions between roflumilast, roflumilast N-oxide and the β2-agonist formoterol with regard to cytokine release by the bronchial preparations. Methods: Bronchial explants from resected lungs were incubated with roflumilast, roflumilast N-oxide and/or formoterol and then stimulated with LPS. An ELISA was used to measure levels of TNF-α and chemokines in the culture supernatants. Results: At a clinically relevant concentration (1 nM), roflumilast N-oxide and roflumilast consistently reduced the release of TNF-α, CCL2, CCL3, CCL4, CCL5 and CXCL9 (but not CXCL1, CXCL5, CXCL8 and IL-6) from human bronchial explants. Formoterol alone decreased the release of TNF-α, CCL2, and CCL3. The combination of formoterol with roflumilast (1 nM) was more potent than roflumilast alone for inhibiting the LPS-induced release of TNF-α, CCL2, CCL3, CCL4, and CXCL9 by the bronchial explants. Conclusions: At a clinically relevant concentration, roflumilast N-oxide and its parent compound, roflumilast, reduced the LPS-induced production of TNF-α and chemokines involved in monocyte and T-cell recruitment but did not alter the release of chemokines involved in neutrophil recruitment. The combination of formoterol with roflumilast enhanced the individual drugs' anti-inflammatory effects.
Keywords: beta-2-adrenoceptor agonist; cytokine; human bronchus; lipopolysaccharide; roflumilast.
Copyright © 2020 Salvator, Buenestado, Brollo, Naline, Victoni, Longchamp, Tenor, Grassin-Delyle and Devillier.
Conflict of interest statement
PD has received consulting fees from Astra Zeneca, Boehringer-Ingelheim, Chiesi, GlaxoSmithKline, Menarini, Mylan, Novartis, and Sanofi. HT is an employee of Topadur. SGD has received a grant from AZ for a clinical trial out of the scope of the present study. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials