

Patterns of Infarction on MRI in Patients With Acute Ischemic Stroke and Cardio-Embolism: A Systematic Review and Meta-Analysis
- PMID: 33363511
- PMCID: PMC7753023
- DOI: 10.3389/fneur.2020.606521
Patterns of Infarction on MRI in Patients With Acute Ischemic Stroke and Cardio-Embolism: A Systematic Review and Meta-Analysis
Abstract
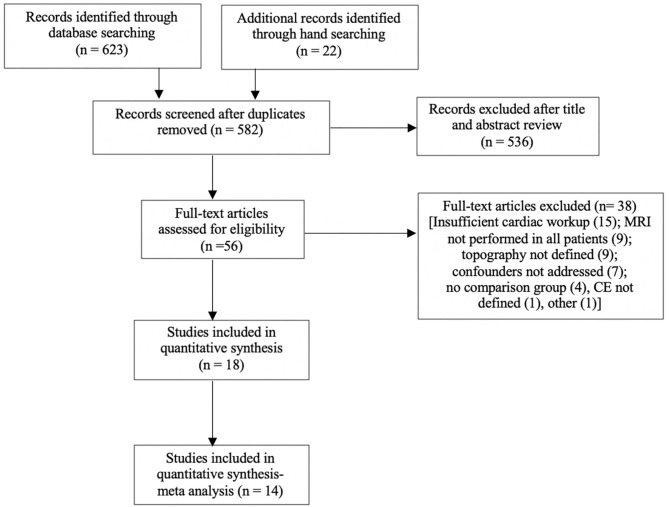
Background: Cardioembolic strokes are common however atrial fibrillation, the most common cause, is often asymptomatic and difficult to detect. There is evidence that infarct topography and volume on magnetic resonance imaging may be associated with specific stroke etiologies. Aim: A systematic review and meta-analysis were undertaken to summarize the available evidence on the association between stroke etiology, infarct topography, and volume. Methods: A systematic review was conducted using Medline (OVID), Embase (OVID), and PubMed databases. Hand searches of the gray literature and of reference lists in relevant articles were also performed. A quality assessment was undertaken, based on the STROBE checklist. For each study, the number of patients with and without a CE source of stroke and infarct topography was collected and outcomes presented as odds ratios (OR) with 95% CI and p-values. Results: Four thousand eight hundred and seventy-three patients with ischemic stroke were included, of whom 1,559 were determined to have a CE source. Bilateral infarcts (OR 3.41; 95% CI 2.20-5.29; p < 0.0001) and multiple territory infarcts (OR 1.57; 95% CI 1.12-2.21; p = 0.009) were more common in patients with a CE source of stroke, than patients without a CE source. Lacunar infarcts (OR 0.49; 95% CI 0.31-0.80; p = 0.004) were more likely to occur in patients without a CE source. No significant difference between the frequency of multiple infarcts (OR 0.96; 95% CI 0.57-1.61; p = 0.87) anterior circulation (OR 1.45; 95% CI 0.83-2.53; p = 0.19) or posterior circulation infarcts (OR 1.06; 95% CI 0.72-1.57; p = 0.75), between the two groups were identified. Three out of four studies examining volume, found a significant association between increased infarct volume and CE source of stroke. A sensitivity analysis with cryptogenic and undetermined stroke sources assumed to be cardioembolic, did not alter the associations observed. Conclusion: The findings of this systematic review and meta-analysis are broadly consistent with previous literature and provide more robust evidence on the association between infarct topography, volume and stroke etiology. Our findings may assist with refining cardiac investigations for patients with cryptogenic stroke, based on infarct topography.
Keywords: cardio-embolism; magnetic resonance imaging; stroke; topography; volume.
Copyright © 2020 Sharobeam, Churilov, Parsons, Donnan, Davis and Yan.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The handling Editor declared a past co-authorship with one of the authors LC.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources