

Fast-Track Ultrasound Clinic for the Diagnosis of Giant Cell Arteritis Changes the Prognosis of the Disease but Not the Risk of Future Relapse
- PMID: 33364248
- PMCID: PMC7753207
- DOI: 10.3389/fmed.2020.589794
Fast-Track Ultrasound Clinic for the Diagnosis of Giant Cell Arteritis Changes the Prognosis of the Disease but Not the Risk of Future Relapse
Abstract
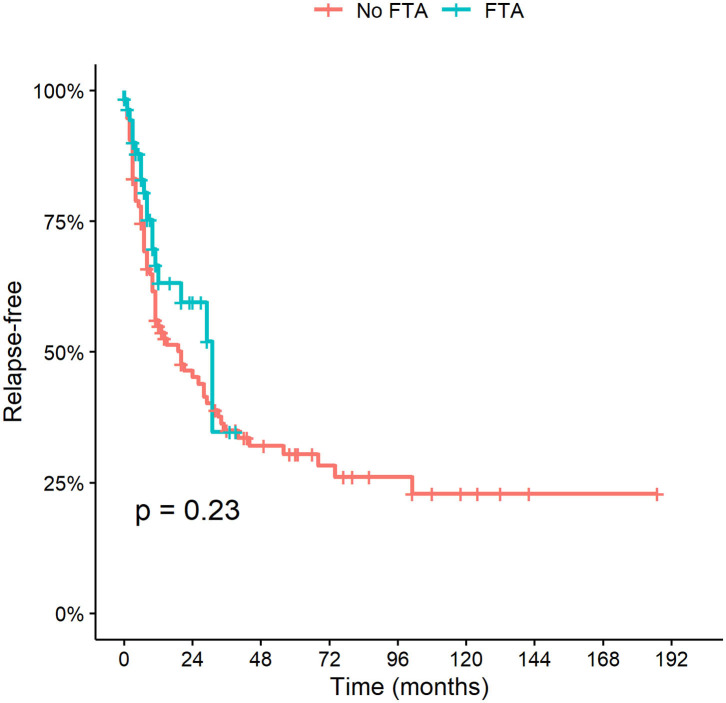
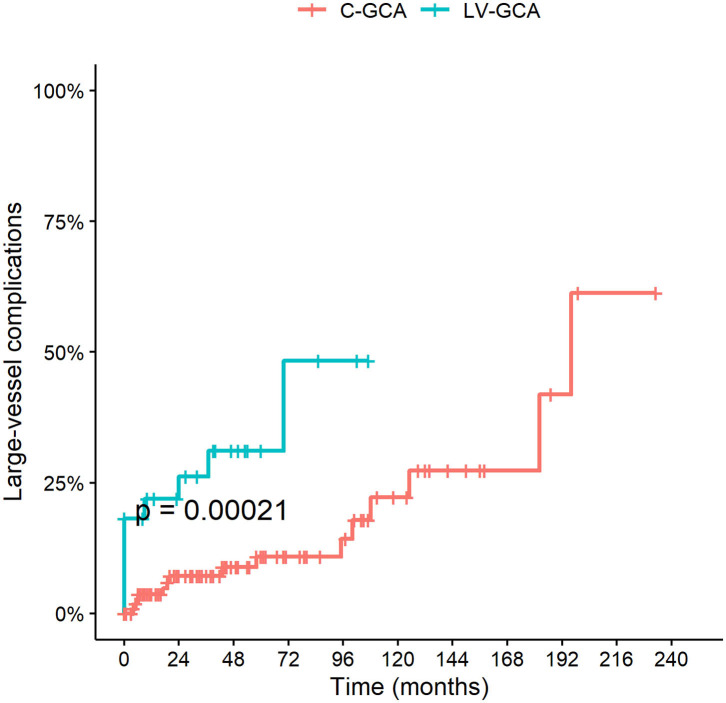
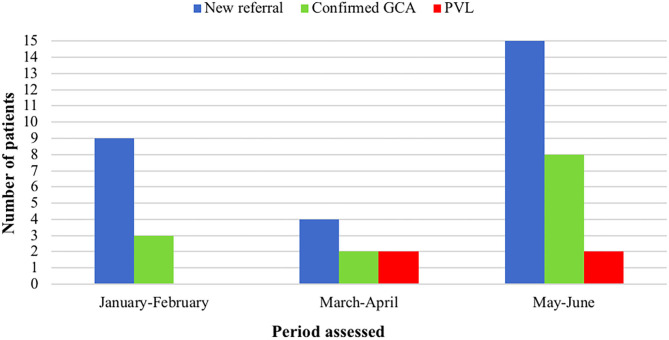
Background: Color Duplex sonography (CDS) of temporal arteries and large vessels (LV) is a recently validated diagnostic methodology for Giant Cell Arteritis (GCA). CDS combined with a fast-track approach (FTA) has improved the early diagnosis of the disease. Objectives: To assess FTA effects on the prevention of permanent visual loss (PVL), relapse and late complications of GCA compared to conventional practice. To assess the impact of COVID-19 pandemic on outcomes of GCA patients assessed with FTA. Methods: GCA patients diagnosed up to June 2020 at the Rheumatology Department, University of Pavia, were included. FTA was implemented since October 2016. FTA consists in the referral within 1 working day of a suspected GCA case to an expert rheumatologist who performs clinical evaluation and CDS. Results: One hundred sixty patients were recruited [female 120 (75%), mean age 72.4 ± 8.2 years]. Sixty-three (39.4%) evaluated with FTA, 97 (60.6%) with conventional approach. FTA patients were older (75.1 ± 7.6 vs. 70.6 ± 8.2 years old; p < 0.001). Median follow-up duration was shorter in the FTA group compared to the conventional one (0.9 vs. 5.0 years; p < 0.001). There was no difference between the two cohorts regarding major vessel district involvement (LV-GCA 17.5% vs. 22.7%; p = 0.4). PVL occurred in 8 (12.7%) FTA patients and 26 (26.8%) conventional ones (p = 0.03). The relative risk of blindness in the conventional group was 2.11 (95% C.I. 1.02-4.36; P = 0.04) as compared to FTA. Median symptom latency of patients experiencing PVL was higher in the conventional group (23 days IQR 12-96 vs. 7 days IQR 4-10, p = 0.02). During COVID-19 there was a significant increase in the occurrence of PVL (40%) including bilateral blindness despite a regularly operating FTA clinic. Cumulative incidence of relapses and time to first relapse did not change after FTA introduction (P = 0.2). No difference in late complications (stenosis/aneurysms) was detected. Conclusions: FTA including CDS evaluation contributed to a substantial reduction of PVL in GCA by shortening the time to diagnosis and treatment initiation. Relapse rate did not change upon FTA introduction, highlighting the need for better disease activity monitoring and treatment strategies optimization based on risk stratification that would predict the occurrence of relapse during glucocorticoid de-escalation.
Keywords: fast-track; giant cell arteritis; large vessel vasculitis; permanent visual loss; sonography; ultrasoud.
Copyright © 2020 Monti, Bartoletti, Bellis, Delvino and Montecucco.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Nuenninghoff DM, Hunder GG, Christianson TJH, McClelland RL, Matteson EL. Incidence and predictors of large-artery complication (aortic aneurysm, aortic dissection, and/or large-artery stenosis) in patients with giant cell arteritis: a population-based study over 50 years. Arthritis Rheum. (2003) 48:3522–31. 10.1002/art.11353 - DOI - PubMed
-
- Patil P, Williams M, Maw WW, Achilleos K, Elsideeg S, Dejaco C, et al. Fast track pathway reduces sight loss in giant cell arteritis: results of a longitudinal observational cohort study. Clin Exp Rheumatol. (2015) 33(2 Suppl. 89):S103–6. - PubMed