

Connective tissue disease-related interstitial lung disease (CTD-ILD) and interstitial lung abnormality (ILA): Evolving concept of CT findings, pathology and management
- PMID: 33364263
- PMCID: PMC7750149
- DOI: 10.1016/j.ejro.2020.100311
Connective tissue disease-related interstitial lung disease (CTD-ILD) and interstitial lung abnormality (ILA): Evolving concept of CT findings, pathology and management
Retraction in
-
Retraction notice to: "Connective tissue disease-related interstitial lung disease (CTD-ILD) and interstitial lung abnormality (ILA): Evolving concept of CT findings, pathology and management" [Eur. J. Radiol. Open 8C (2021) 100311].Eur J Radiol Open. 2022 Feb 11;9:100402. doi: 10.1016/j.ejro.2022.100402. eCollection 2022. Eur J Radiol Open. 2022. PMID: 36619809 Free PMC article.
Abstract
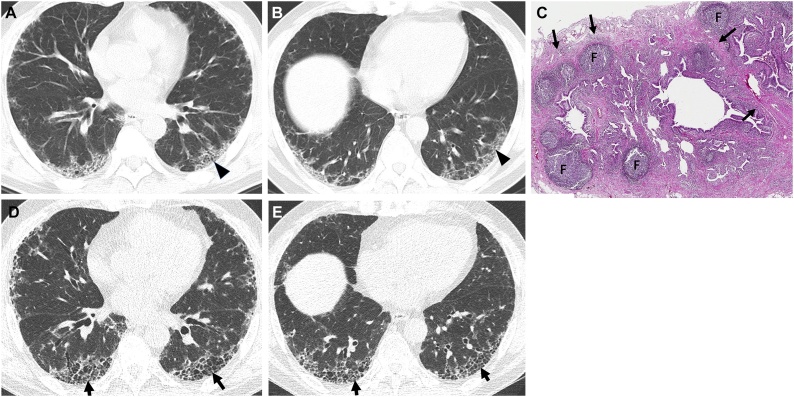
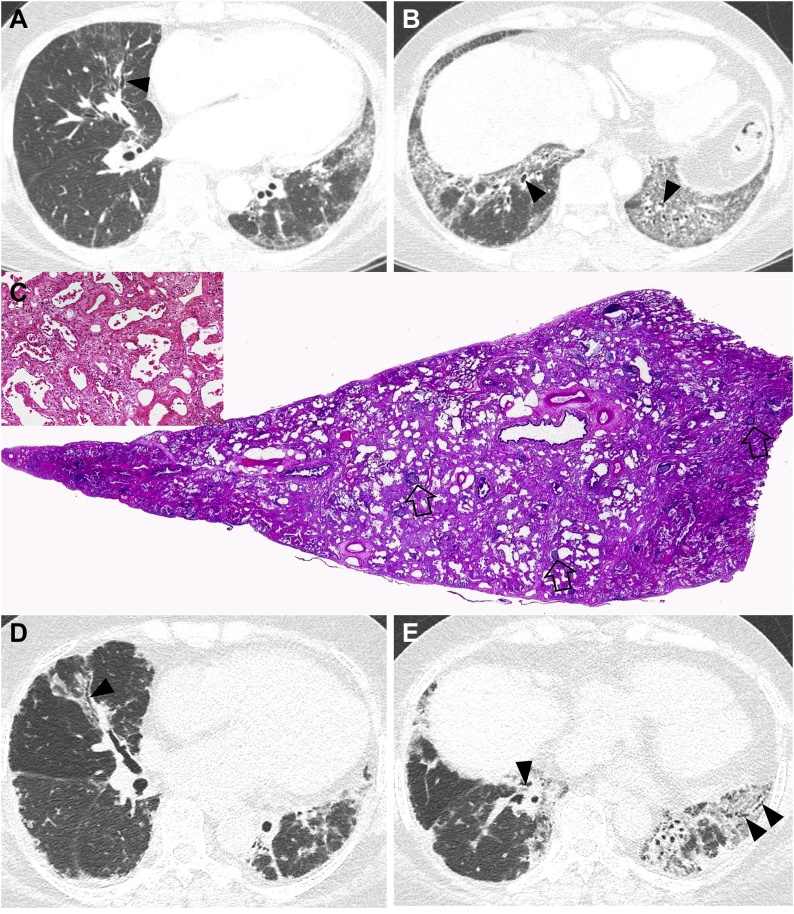
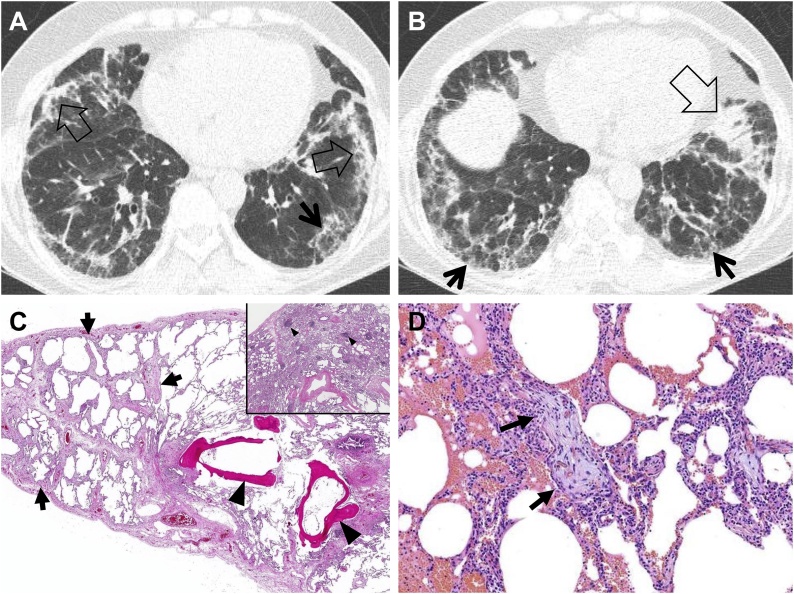
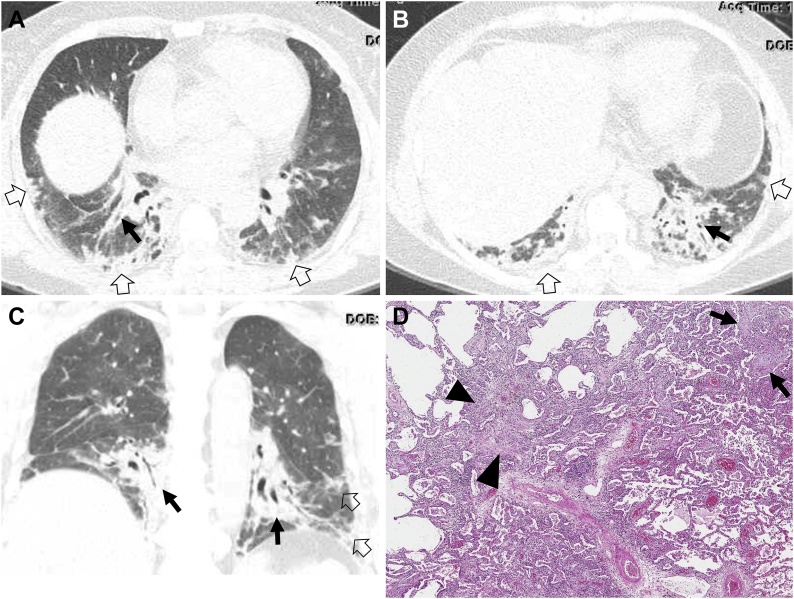
The connective tissue diseases (CTDs) demonstrating features of interstitial lung disease (ILD) include systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), progressive systemic sclerosis (PSS), dermatomyositis (DM) and polymyositis (PM), ankylosing spondylitis (AS), Sjogren's syndrome (SS), and mixed connective tissue disease (MCTD). In RA patients in particular, interstitial lung abnormality (ILA) (of varying degrees; severe vs. mild) is reported to occur in approximately 20-60 % of individuals and CT disease progression occurs in approximately 35-45 % of them. The ILAs have been associated with a spectrum of functional and physiologic decrement. The identification of progressive ILA may enable appropriate surveillance and the commencement of treatment with the goal of improving morbidity and mortality rates of established RA-ILD. Subpleural distribution and higher baseline ILA/ILD extent were risk factors associated with disease progression. At histopathologic analysis, connective tissue disease-related interstitial lung diseases (CTD-ILDs) are diverse and include nonspecific interstitial pneumonia (NSIP), usual interstitial pneumonia (UIP), organizing pneumonia (OP), apical fibrosis, diffuse alveolar damage (DAD), and lymphoid interstitial pneumonia (LIP). Even though proportions of ILDs vary, NSIP pattern accounts for a large proportion, especially in PSS, DM/PM and MCTD, followed by UIP pattern. Evidence has been published that treatment of subclinical CT lung abnormalities showing a tendency to progress to ILD may stabilize the CT alterations. The identification of subclinical lung abnormalities can be appropriate in the management of the disease and CT appears to be the gold standard for the evaluation of lung parenchyma.
Keywords: CTD, Connective tissue disease; CTD-ILD, (Connective Tissue Disease-Related Interstitial Lung Disease); Connective tissue disease; DM, Dermatomyositis; IIP, Idiopathic interstitial pneumonia; ILA, Interstitial lung abnormality; ILD, Interstitial lung disease; IPAF, Interstitial pneumonitis with autoimmune features; IPF, Idiopathic pulmonary fibrosis; Interstitial lung abnormality; Interstitial lung disease; MCTD, Mixed connective tissue disease; NSIP, Nonspecific Interstitial Pneumonia; OP, Organizing pneumonia; PM, Polymyositis; PSS, Progressive Systemic Sclerosis; RA, Rheumatoid Arthritis; SLE, Systemic Lupus Erythematosus; SS, Sjogren’s Syndrome; UCTD, Undifferentiated Connective Tissue Disease; UIP, Usual Interstitial Pneumonia.
© 2020 The Authors.
Conflict of interest statement
The authors report no declarations of interest.
Figures
References
-
- American Thoracic Society, European Respiratory Society, American Thoracic Society/European Respiratory Society International Multidisciplinary Consensus Classification of the Idiopathic Interstitial Pneumonias This joint statement of the American Thoracic Society (ATS), and the European Respiratory Society (ERS) was adopted by the ATS board of directors, June 2001 and by the ERS Executive Committee, June 2001. Am. J. Respir. Crit. Care Med. 2002;165:277–304. - PubMed
-
- Lederer D.J., Martinez F.J. Idiopathic pulmonary fibrosis. N. Engl. J. Med. 2018;378:1811–1823. - PubMed
-
- Jeganathan N., Sathananthan M. Connective tissue disease-related interstitial lung disease: prevalence, patterns, predictors, prognosis, and treatment. Lung. 2020;198:735–759. - PubMed
-
- Ng K.H., Chen D.Y., Lin C.H., Chao W.C., Chen Y.M., Chen Y.H., Huang W.N., Hsieh T.Y., Lai K.L., Tang K.T., Chen H.H. Risk of interstitial lung disease in patients with newly diagnosed systemic autoimmune rheumatic disease: a nationwide, population-based cohort study. Semin. Arthritis Rheum. 2020;50:840–845. - PubMed
-
- Kim E.A., Lee K.S., Johkoh T., Kim T.S., Suh G.Y., Kwon O.J., Han J. Interstitial lung diseases associated with collagen vascular diseases: radiologic and histopathologic findings. Radiographics. 2002;22:S151–165. Spec No. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
