

Laryngeal complications of COVID-19
- PMID: 33364402
- PMCID: PMC7752067
- DOI: 10.1002/lio2.484
Laryngeal complications of COVID-19
Abstract
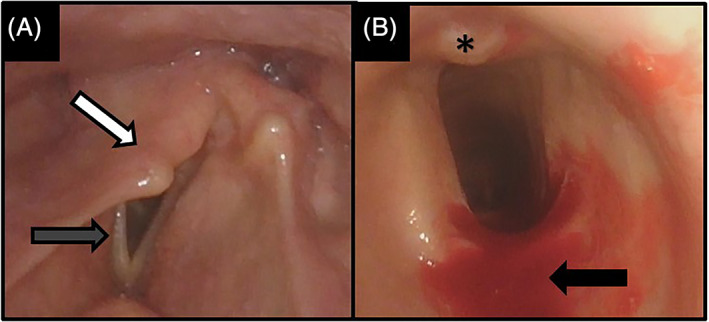
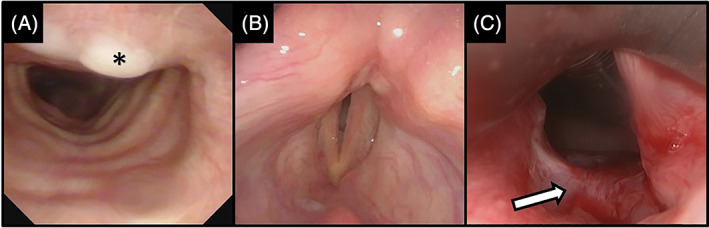
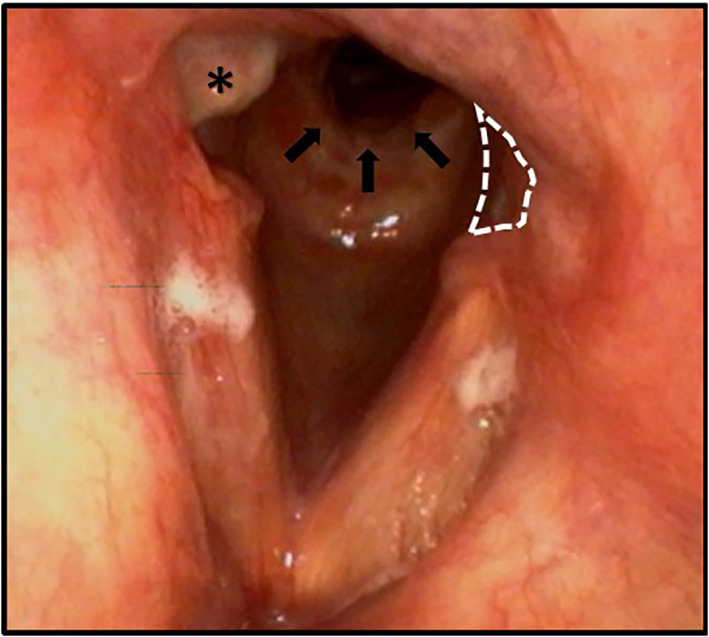
Objective: To describe and visually depict laryngeal complications in patients recovering from coronavirus disease 2019 (COVID-19) infection along with associated patient characteristics.
Study design: Prospective patient series.
Setting: Tertiary laryngology care centers.
Subjects and methods: Twenty consecutive patients aged 18 years or older presenting with laryngological complaints following recent COVID-19 infection were included. Patient demographics, comorbid medical conditions, COVID-19 diagnosis dates, symptoms, intubation, and tracheostomy status, along with subsequent laryngological symptoms related to voice, airway, and swallowing were collected. Findings on laryngoscopy and stroboscopy were included, if performed.
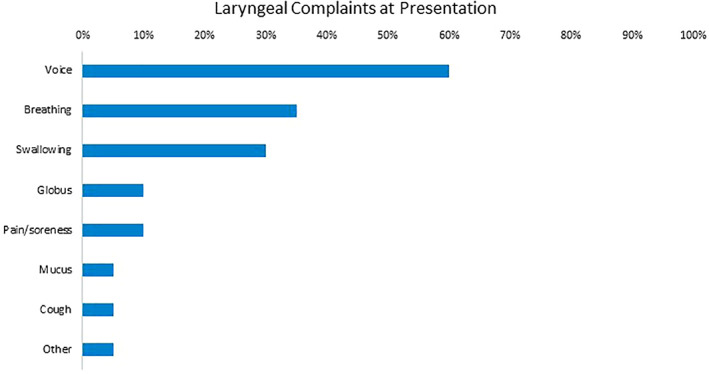
Results: Of the 20 patients enrolled, 65% had been intubated for an average duration of 21.8 days and 69.2% requiring prone-position mechanical ventilation. Voice-related complaints were the most common presenting symptom, followed by those related to swallowing and breathing. All patients who underwent flexible laryngoscopy demonstrated laryngeal abnormalities, most frequently in the glottis (93.8%), and those who underwent stroboscopy had abnormalities in mucosal wave (87.5%), periodicity (75%), closure (50%), and symmetry (50%). Unilateral vocal fold immobility was the most common diagnosis (40%), along with posterior glottic (15%) and subglottic (10%) stenoses. 45% of patients underwent further procedural intervention in the operating room or office. Many findings were suggestive of intubation-related injury.
Conclusion: Prolonged intubation with prone-positioning commonly employed in COVID-19 respiratory failure can lead to significant laryngeal complications with associated difficulties in voice, airway, and swallowing. The high percentage of glottic injuries underscores the importance of stroboscopic examination. Otolaryngologists must be prepared to manage these complications in patients recovering from COVID-19.
Level of evidence: IV.
Keywords: COVID‐19; intubation; laryngology; larynx; stenosis; voice.
© 2020 The Authors. Laryngoscope Investigative Otolaryngology published by Wiley Periodicals LLC on behalf of The Triological Society.
Conflict of interest statement
The authors declare no potential conflict of interest.
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials