

Twin study confirms virtually identical prenatal alcohol exposures can lead to markedly different fetal alcohol spectrum disorder outcomes-fetal genetics influences fetal vulnerability
- PMID: 33364429
- PMCID: PMC7757639
- DOI: 10.24105/apr.2019.5.23
Twin study confirms virtually identical prenatal alcohol exposures can lead to markedly different fetal alcohol spectrum disorder outcomes-fetal genetics influences fetal vulnerability
Abstract
Background: Risk of fetal alcohol spectrum disorder (FASD) is not based solely on the timing and level of prenatal alcohol exposure (PAE). The effects of teratogens can be modified by genetic differences in fetal susceptibility and resistance. This is best illustrated in twins.
Objective: To compare the prevalence and magnitude of pairwise discordance in FASD diagnoses across monozygotic twins, dizygotic twins, full-siblings, and half-siblings sharing a common birth mother.
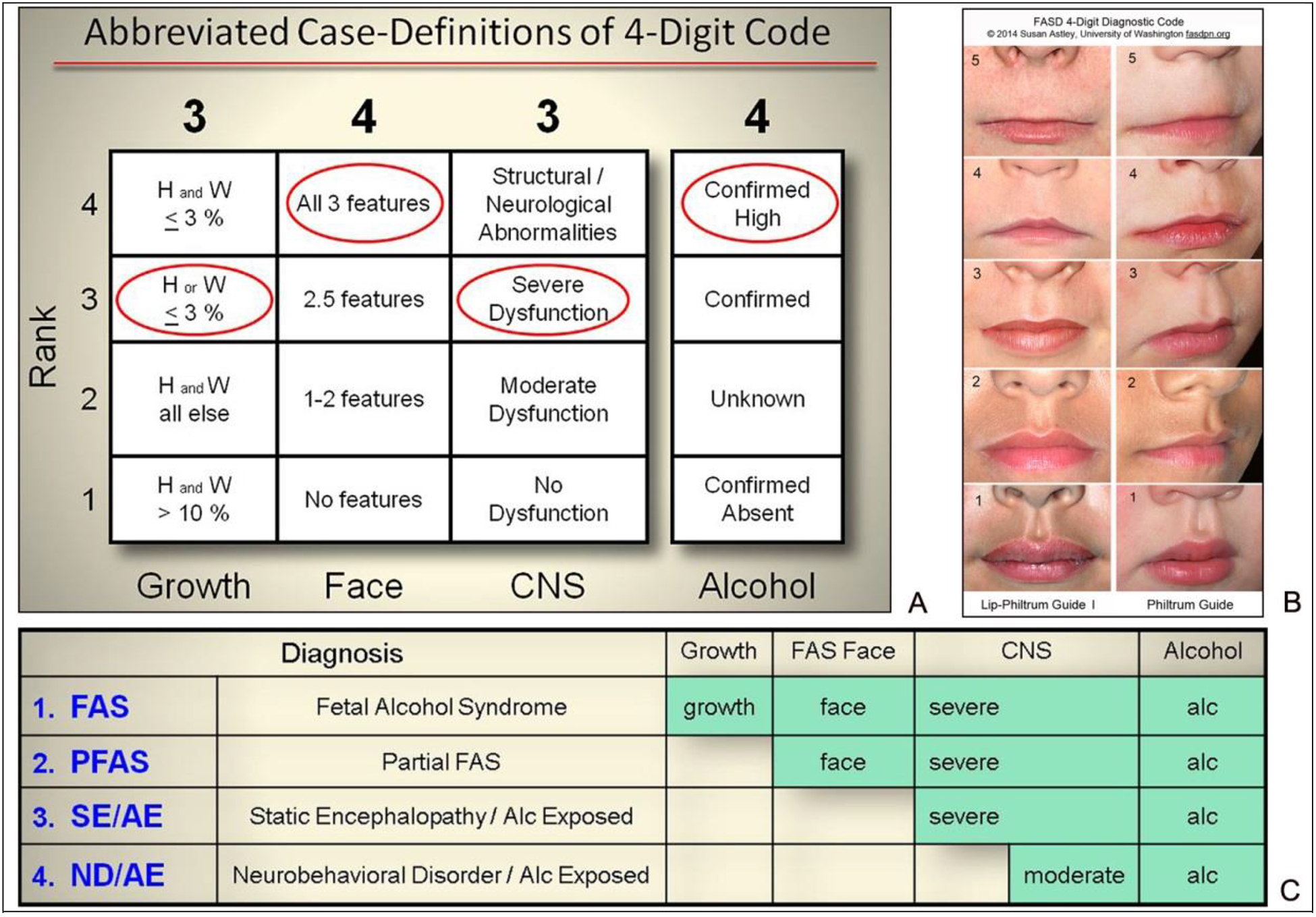
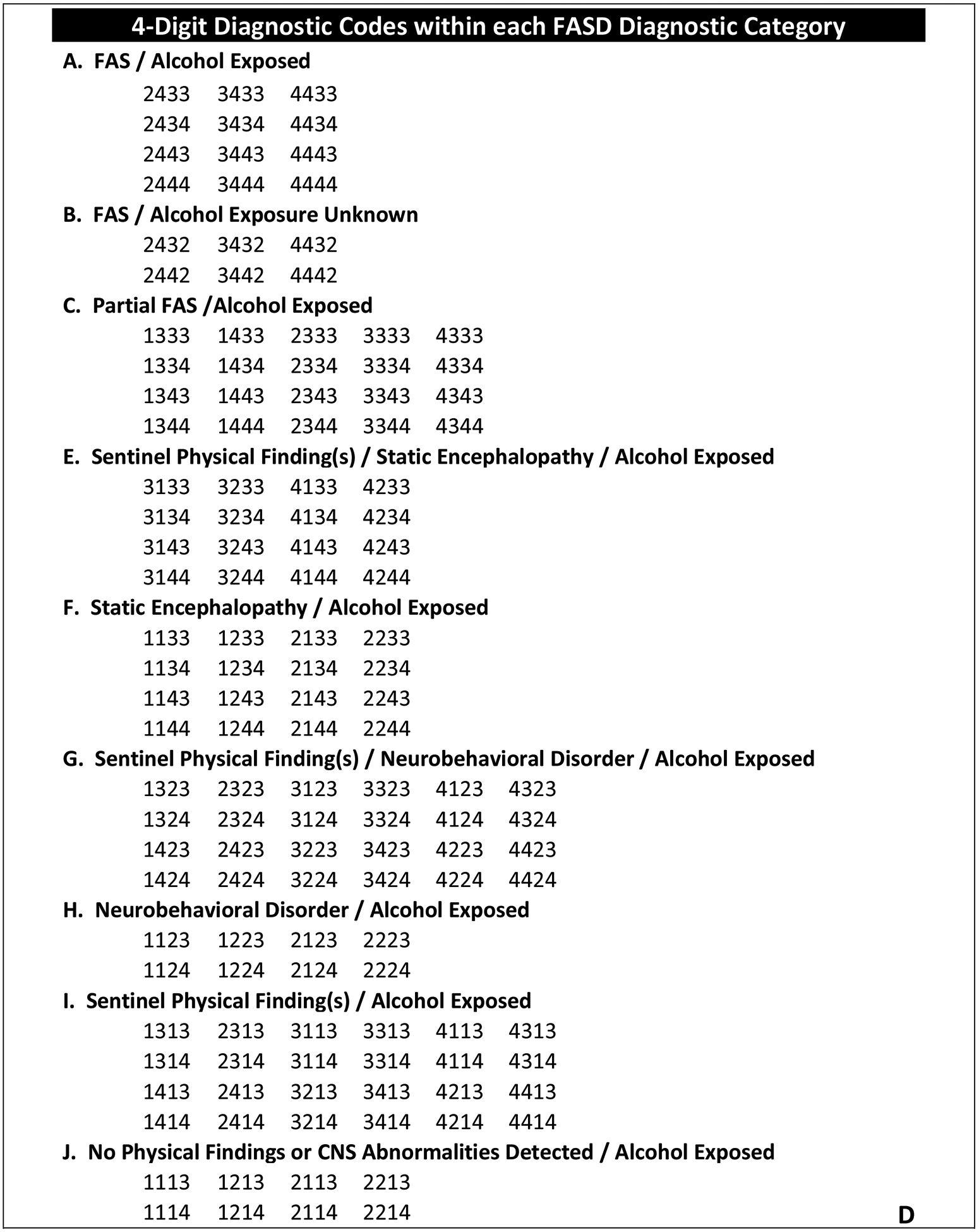
Methods: Data from the Fetal Alcohol Syndrome Diagnostic & Prevention Network clinical database was used. Sibling pairs were matched on age and PAE, raised together, and diagnosed by the same University of Washington interdisciplinary team using the FASD 4-Digit Code. This design sought to assess and isolate the role of genetics on fetal vulnerability/resistance to the teratogenic effects of PAE by eliminating or minimizing pairwise discordance in PAE and other prenatal/postnatal risk factors.
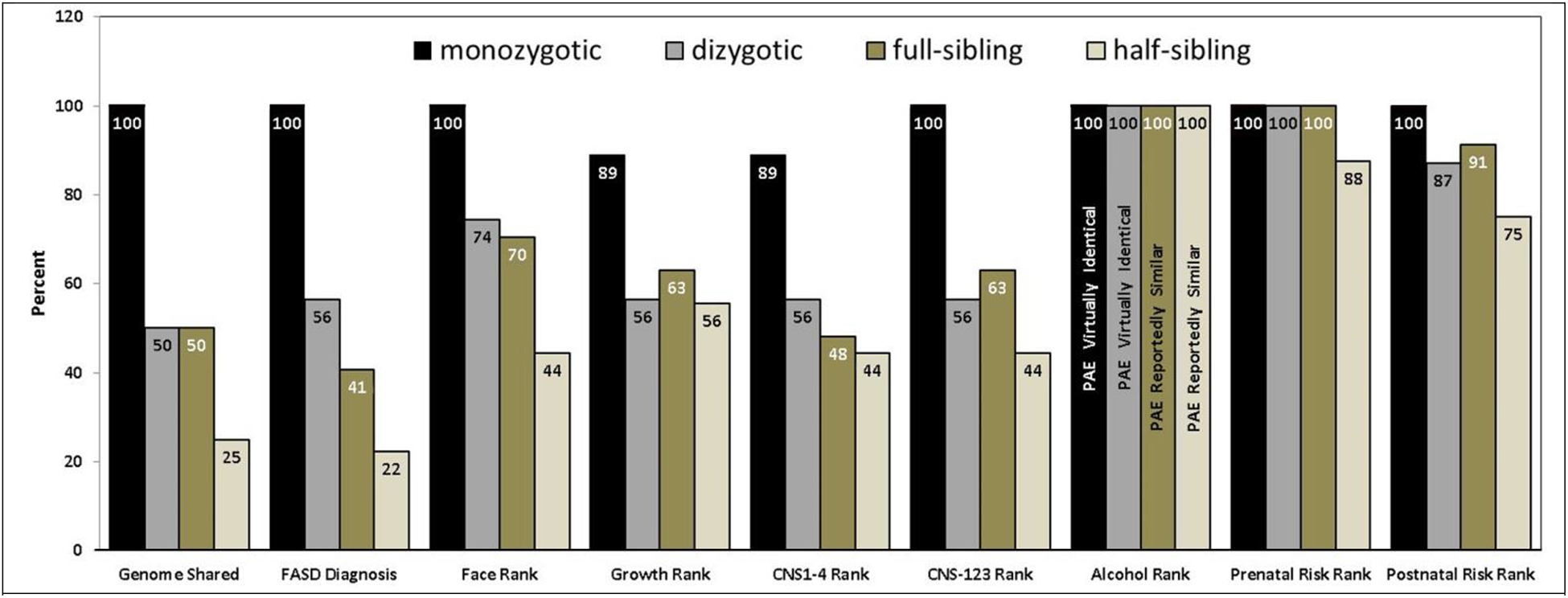
Results: As genetic relatedness between siblings decreased from 100% to 50% to 50% to 25% across the four groups (9 monozygotic, 39 dizygotic, 27 full-sibling and 9 half-sibling pairs, respectively), the prevalence of pairwise discordance in FASD diagnoses increased from 0% to 44% to 59% to 78%. Despite virtually identical PAE, 4 pairs of dizygotic twins had FASD diagnoses at opposite ends of the fetal alcohol spectrum-Partial Fetal Alcohol Syndrome versus Neurobehavioral Disorder/Alcohol-Exposed.
Conclusion: Despite virtually identical PAE, fetuses can experience vastly different FASD outcomes. Thus, to protect all fetuses, especially the most genetically vulnerable, the only safe amount to drink is none at all.
Keywords: fetal alcohol spectrum disorder; genetics; prenatal alcohol exposure; twins.
Figures
References
-
- Wilson JG. Current Status of Teratology: General principles and mechanisms derived from animal studies In Wilson JG, Fraser FC (eds): “Handbook of Teratology, Vol. 1, General Principles and Etiology” London: Plenum Press, London, pp 47–74, 1977
-
- Astley SJ. Diagnostic Guide for Fetal Alcohol Spectrum Disorders: The 4-Digit Diagnostic Code, 3rd ed., Seattle WA, University of Washington Publication Services; 2004. Available from: http://depts.washington.edu/fasdpn/pdfs/guide04.pdf
-
- Astley SJ, Clarren SK. Diagnosing the full spectrum of fetal alcohol exposed individuals: Introducing the 4-Digit Diagnostic Code. Alcohol Alcohol. 2000;35:400–410. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials