

Aspirin and heparin in the treatment of recurrent spontaneous abortion associated with antiphospholipid antibody syndrome: A systematic review and meta-analysis
- PMID: 33365057
- PMCID: PMC7716630
- DOI: 10.3892/etm.2020.9489
Aspirin and heparin in the treatment of recurrent spontaneous abortion associated with antiphospholipid antibody syndrome: A systematic review and meta-analysis
Abstract
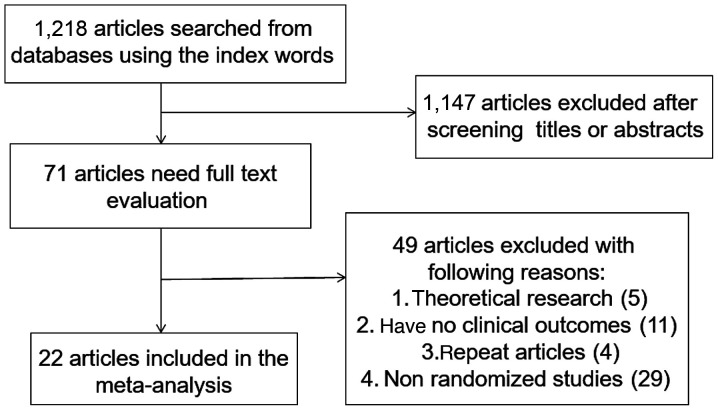
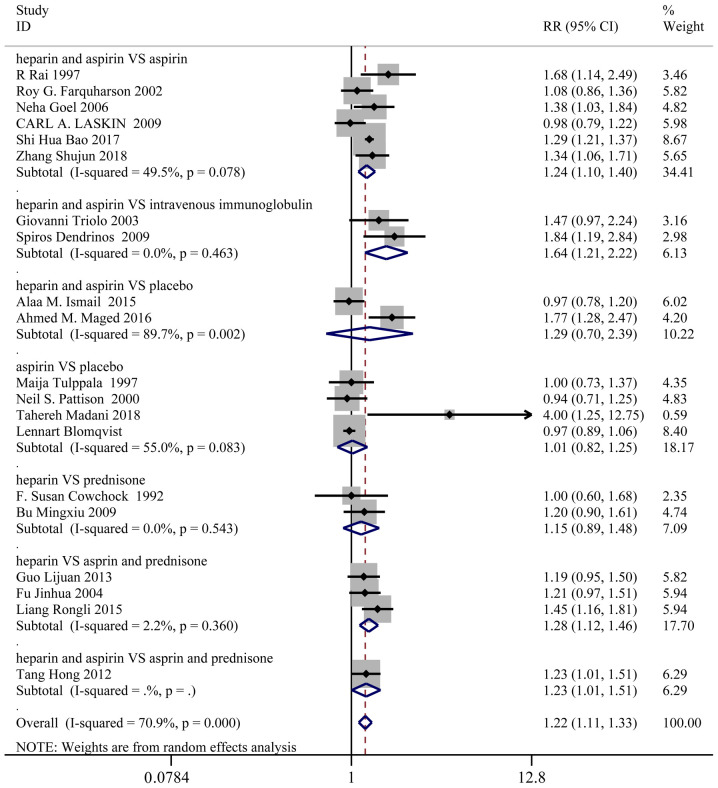
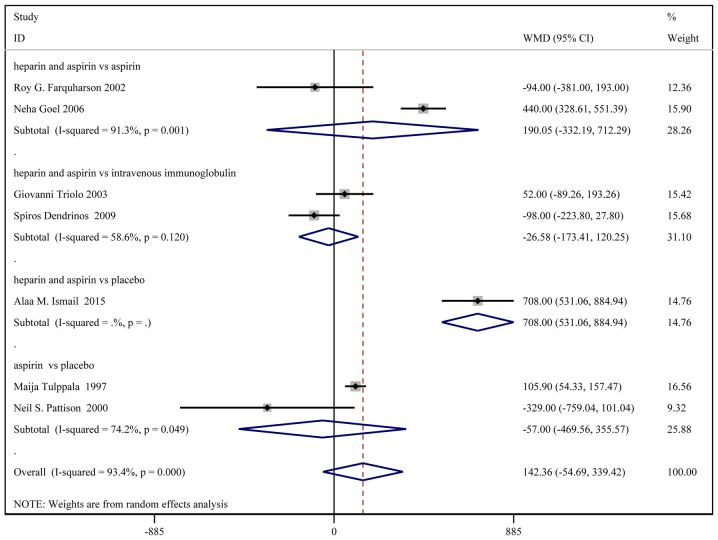
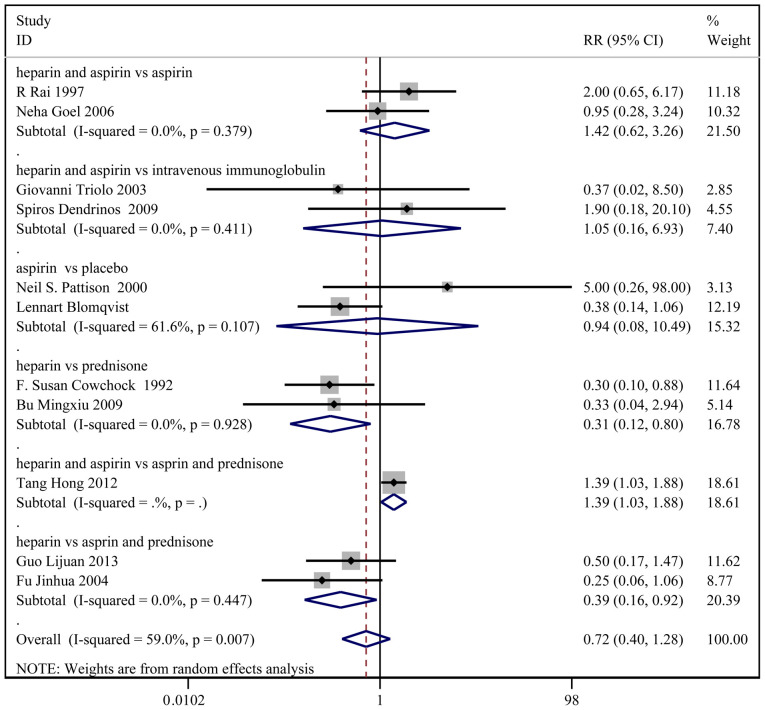
The present study aimed to review relevant, randomized, controlled trials in order to determine the effects of aspirin and heparin treatment on recurrent spontaneous abortion (RSA) in women with antiphospholipid syndrome (APS). Previous relevant studies were identified using PubMed, Cochrane, Embase, CNKI, VANFUN and VIP by retrieving appropriate key words. Additionally, key relevant sources in the literature were reviewed and articles published before May 2019 were included. The 22 selected studies included 1,515 patients in the treatment group and 1,531 patients in the control group. These previous studies showed that heparin and aspirin significantly improved live birth rate when compared with treatments using intravenous immunoglobulin, aspirin alone or aspirin combined with prednisone. Moreover, heparin and aspirin greatly increased the birth weight compared with placebo and improved vaginal delivery relative to intravenous immunoglobulin. The gestational age at birth was significantly higher in the heparin and aspirin group compared with the placebo group and the incidence of intrauterine growth restriction was lower in the heparin and aspirin group compared with the placebo group. Furthermore, heparin and aspirin markedly reduced the incidence of miscarriage compared with the aspirin group and the placebo group, and the incidence of pre-eclampsia was lower in the heparin and aspirin group than the placebo group. Thus, heparin and aspirin could be further examined for the treatment of RSA in women with APS.
Keywords: antiphospholipid syndrome; aspirin; heparin; meta-analysis; recurrent spontaneous abortion.
Copyright: © Yu et al.
Figures
Similar articles
-
Aspirin or heparin or both in the treatment of recurrent spontaneous abortion in women with antiphospholipid antibody syndrome: a meta-analysis of randomized controlled trials.J Matern Fetal Neonatal Med. 2019 Apr;32(8):1299-1311. doi: 10.1080/14767058.2017.1404979. Epub 2018 Jan 10. J Matern Fetal Neonatal Med. 2019. PMID: 29179589
-
Aspirin or heparin or both for improving pregnancy outcomes in women with persistent antiphospholipid antibodies and recurrent pregnancy loss.Cochrane Database Syst Rev. 2020 May 2;5(5):CD012852. doi: 10.1002/14651858.CD012852.pub2. Cochrane Database Syst Rev. 2020. PMID: 32358837 Free PMC article.
-
Prevention of recurrent miscarriage in women with antiphospholipid syndrome: A systematic review and network meta-analysis.Lupus. 2021 Jan;30(1):70-79. doi: 10.1177/0961203320967097. Epub 2020 Oct 20. Lupus. 2021. PMID: 33081590
-
Meta-analysis on aspirin combined with low-molecular-weight heparin for improving the live birth rate in patients with antiphospholipid syndrome and its correlation with d-dimer levels.Medicine (Baltimore). 2021 Jun 25;100(25):e26264. doi: 10.1097/MD.0000000000026264. Medicine (Baltimore). 2021. PMID: 34160390 Free PMC article.
-
Meta-analysis of heparin combined with aspirin versus aspirin alone for unexplained recurrent spontaneous abortion.Int J Gynaecol Obstet. 2020 Oct;151(1):23-32. doi: 10.1002/ijgo.13266. Epub 2020 Jul 4. Int J Gynaecol Obstet. 2020. PMID: 32535924
Cited by
-
Maternal and perinatal outcomes of low-dose aspirin plus low-molecular-weight heparin therapy on antiphospholipid antibody-positive pregnant women with chronic hypertension.Front Pediatr. 2023 May 5;11:1148547. doi: 10.3389/fped.2023.1148547. eCollection 2023. Front Pediatr. 2023. PMID: 37215604 Free PMC article.
-
Application Value of Combined Detection of Anti-β2-GPI, ACL, and Lupus Anticoagulant in the Diagnosis of Patients with Antiphospholipid Syndrome.Evid Based Complement Alternat Med. 2022 Nov 3;2022:9377334. doi: 10.1155/2022/9377334. eCollection 2022. Evid Based Complement Alternat Med. 2022. Retraction in: Evid Based Complement Alternat Med. 2023 Jul 19;2023:9873756. doi: 10.1155/2023/9873756. PMID: 36387368 Free PMC article. Retracted.
-
British Society for Rheumatology guideline on prescribing drugs in pregnancy and breastfeeding: comorbidity medications used in rheumatology practice.Rheumatology (Oxford). 2023 Apr 3;62(4):e89-e104. doi: 10.1093/rheumatology/keac552. Rheumatology (Oxford). 2023. PMID: 36318967 Free PMC article. No abstract available.
-
Executive Summary: British Society for Rheumatology guideline on prescribing drugs in pregnancy and breastfeeding: comorbidity medications used in rheumatology practice.Rheumatology (Oxford). 2023 Apr 3;62(4):1388-1397. doi: 10.1093/rheumatology/keac559. Rheumatology (Oxford). 2023. PMID: 36318970 Free PMC article. No abstract available.
-
Off-label indications of aspirin in gynaecology and obstetrics outpatients at two Chinese tertiary care hospitals: a retrospective cross-sectional study.BMJ Open. 2022 Feb 21;12(2):e050702. doi: 10.1136/bmjopen-2021-050702. BMJ Open. 2022. PMID: 35190417 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous