

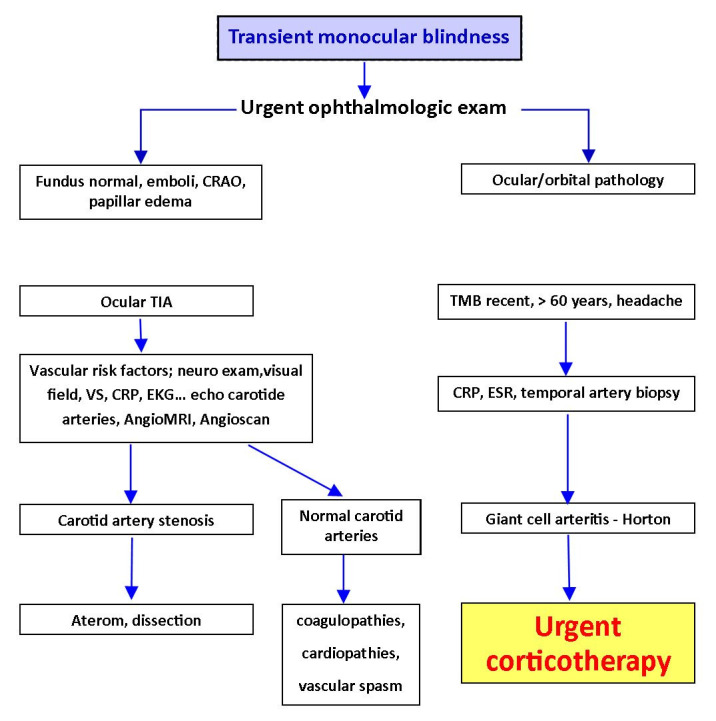
Vascular emergencies in neuro-ophthalmology
- PMID: 33367170
- PMCID: PMC7739024
- DOI: 10.22336/rjo.2020.54
Vascular emergencies in neuro-ophthalmology
Abstract
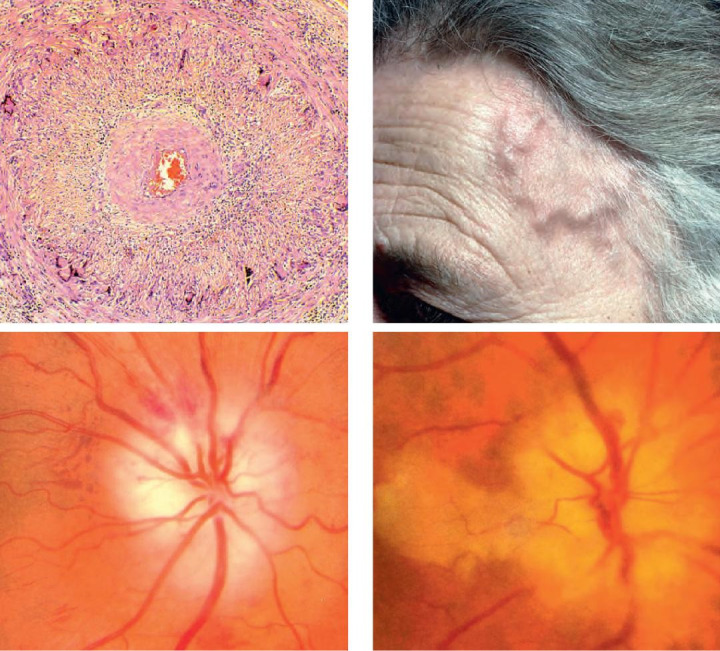
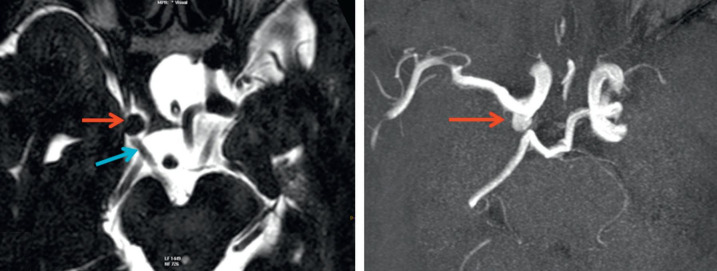
The cerebral vascularization is assured by the 2 internal carotids and 2 vertebral arteries, and the Willis circle. Carotid artery obstruction is the most common abnormality associated with ocular ischemic syndrome. Obstruction may be due to atheromatous plaque, external compression, arteritis, or dissection of the artery. An atheromatous lesion of the carotid artery is the most frequent lesion responsible for ocular ischemic syndrome. The signs and symptoms of ocular ischemic syndrome are associated with severe hypoperfusion of the eye. Inflammatory lesions of the carotid artery are responsible for decreased flow in the carotid system. Other vascular emergencies are carotid artery dissection, Horton arteritis, aneurysms and carotid-cavernous fistula. The most common ocular signs and symptoms are transient monocular blindness, persistent monocular blindness, ocular ischemia, Claude Bernard Horner syndrome and oculomotor palsies. The carotid pathology can be a life-threatening pathology and it is important to recognize all these signs and symptoms. A multi-specialty approach will prevent misdiagnosis and lead to a better patient management. Abbreviations: OIS = ocular ischemic syndrome, TMB = transient monocular blindness, TIA = transient ischemic attack, ESR = erythrocyte sedimentation rate, CRP = C reactive protein, NVE = neovascularization elsewhere in the retina, NVD = neovascularization on the disc, AION A = anterior ischemic arteritic optic neuropathy, CBH = Claude Bernard Horner syndrome, MRI = magnetic resonance imaging.
Keywords: Claude Bernard Horner syndrome; carotid artery stenosis; ocular ischemic syndrome; oculomotor palsies; transient monocular blindness.
©Romanian Society of Ophthalmology.
Figures






References
-
- Rea P. Blood Supply of the Brain and Clinical Issues. Essential Clinical Anatomy of the Nervous System. 2015
-
- Ashrafian H. Anatomically specific clinical examination of the carotid arterial tree. Anatomical Science International. 2007 Mar;82(1):16–23. - PubMed
-
- Brown GC, Green WR. The ocular ischaemic syndrome. Curr Opinion Ophthalmol. 1994;5:14–20.
-
- Crassard I. Oeil. Pathologie carotid et vertebrobasilaire. DU Neuro-ophtalmologie. Paris: 2018-2019.
-
- Solomon CG, Grotta JC. Carotid Stenosis. New England Journal of Medicine. 2013;369(12):1143–1150. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous