

Recent Smell Loss Is the Best Predictor of COVID-19 Among Individuals With Recent Respiratory Symptoms
- PMID: 33367502
- PMCID: PMC7799216
- DOI: 10.1093/chemse/bjaa081
Recent Smell Loss Is the Best Predictor of COVID-19 Among Individuals With Recent Respiratory Symptoms
Abstract
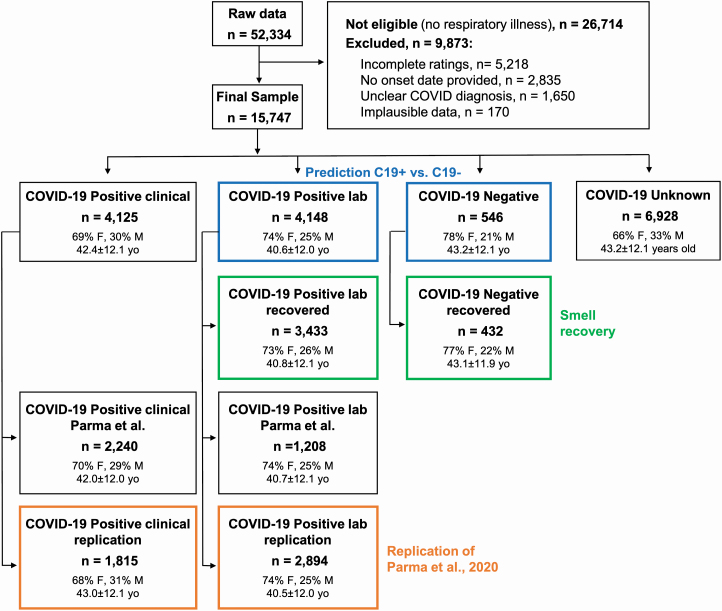
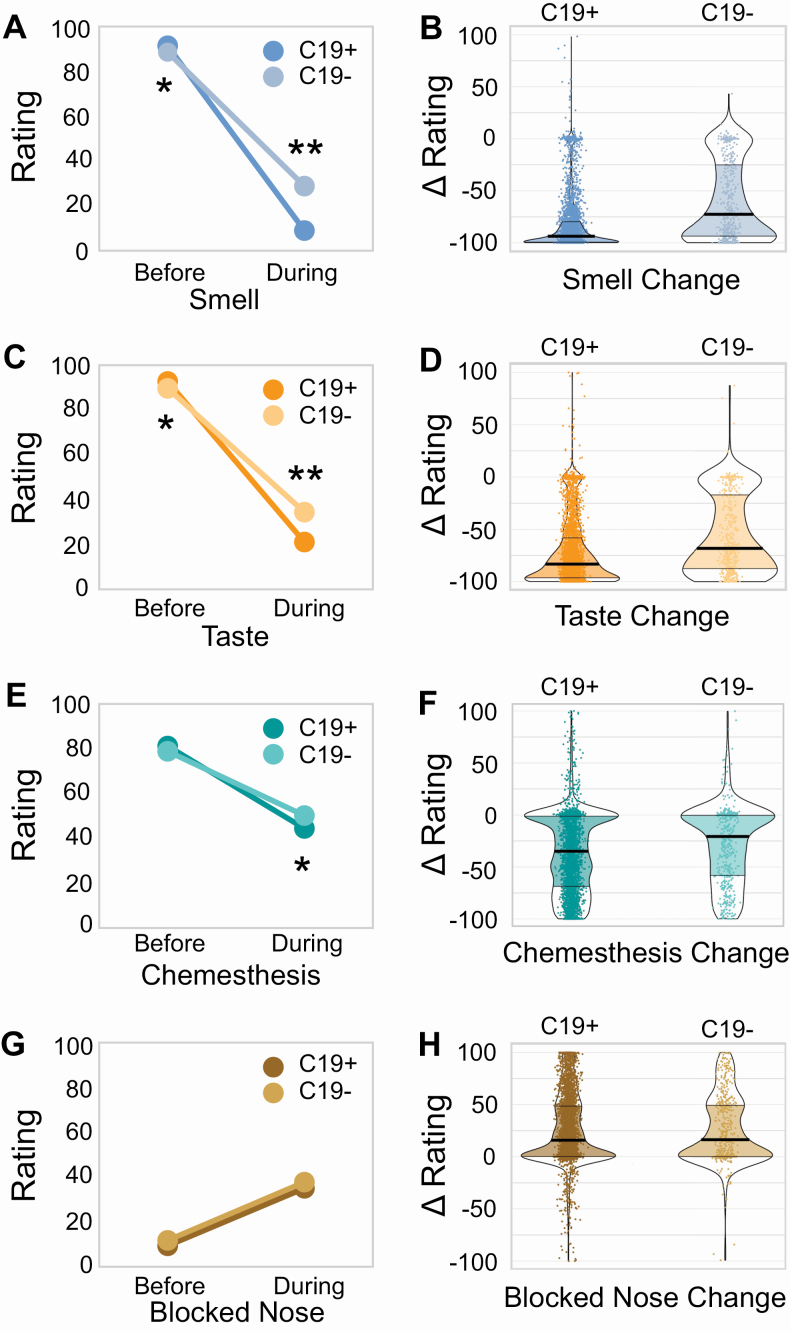
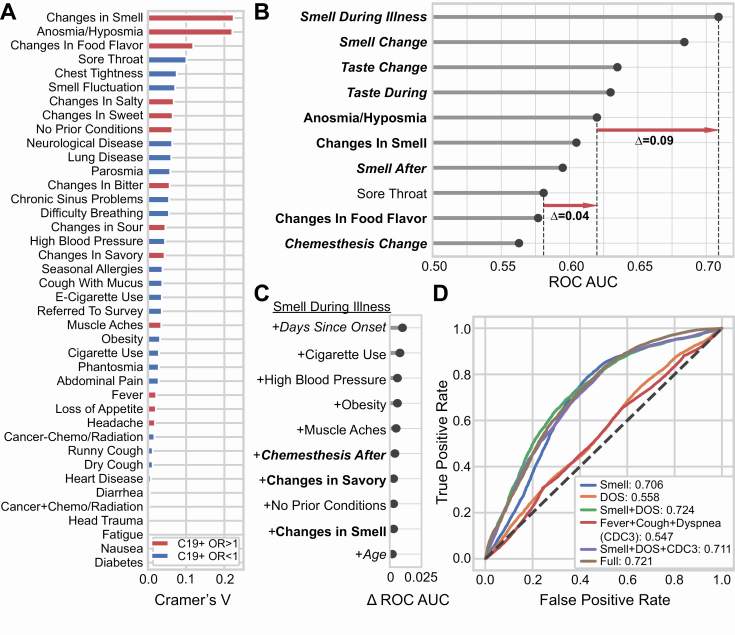
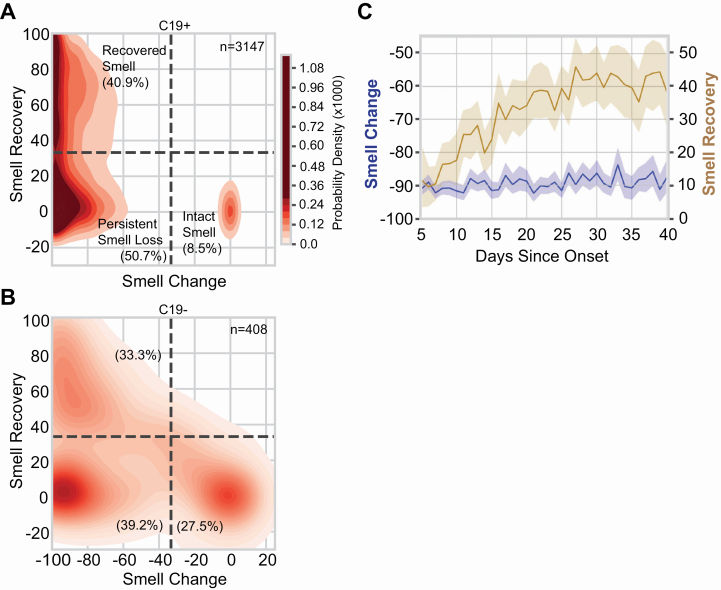
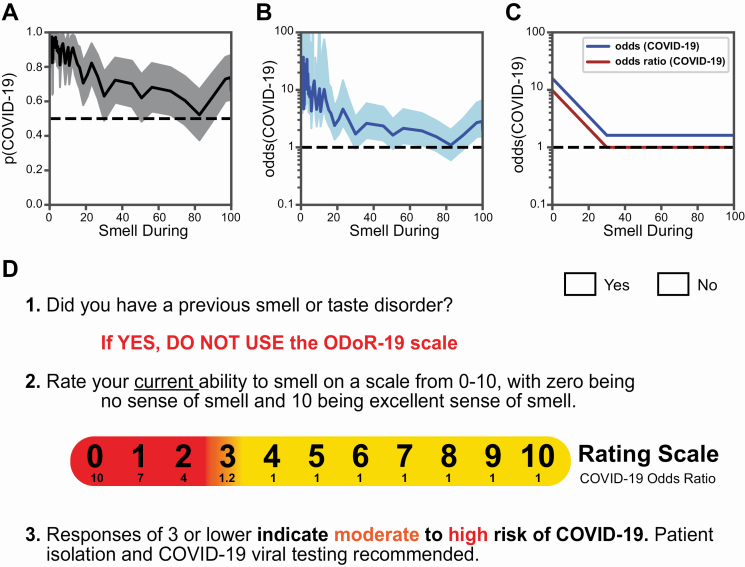
In a preregistered, cross-sectional study, we investigated whether olfactory loss is a reliable predictor of COVID-19 using a crowdsourced questionnaire in 23 languages to assess symptoms in individuals self-reporting recent respiratory illness. We quantified changes in chemosensory abilities during the course of the respiratory illness using 0-100 visual analog scales (VAS) for participants reporting a positive (C19+; n = 4148) or negative (C19-; n = 546) COVID-19 laboratory test outcome. Logistic regression models identified univariate and multivariate predictors of COVID-19 status and post-COVID-19 olfactory recovery. Both C19+ and C19- groups exhibited smell loss, but it was significantly larger in C19+ participants (mean ± SD, C19+: -82.5 ± 27.2 points; C19-: -59.8 ± 37.7). Smell loss during illness was the best predictor of COVID-19 in both univariate and multivariate models (ROC AUC = 0.72). Additional variables provide negligible model improvement. VAS ratings of smell loss were more predictive than binary chemosensory yes/no-questions or other cardinal symptoms (e.g., fever). Olfactory recovery within 40 days of respiratory symptom onset was reported for ~50% of participants and was best predicted by time since respiratory symptom onset. We find that quantified smell loss is the best predictor of COVID-19 amongst those with symptoms of respiratory illness. To aid clinicians and contact tracers in identifying individuals with a high likelihood of having COVID-19, we propose a novel 0-10 scale to screen for recent olfactory loss, the ODoR-19. We find that numeric ratings ≤2 indicate high odds of symptomatic COVID-19 (4 < OR < 10). Once independently validated, this tool could be deployed when viral lab tests are impractical or unavailable.
Keywords: anosmia; chemosensory; coronavirus; hyposmia; olfactory; prediction.
© The Author(s) 2020. Published by Oxford University Press. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Update of
-
The best COVID-19 predictor is recent smell loss: a cross-sectional study.medRxiv [Preprint]. 2020 Jul 28:2020.07.22.20157263. doi: 10.1101/2020.07.22.20157263. medRxiv. 2020. Update in: Chem Senses. 2021 Jan 1;46:bjaa081. doi: 10.1093/chemse/bjaa081. PMID: 32743605 Free PMC article. Updated. Preprint.
References
-
- CDC. 2020. Coronavirus disease 2019 (COVID-19) – symptoms. Available from: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html.
-
- Croy I, Nordin S, Hummel T. 2014. Olfactory disorders and quality of life – an updated review. Chem Senses. 39(3):185–194. - PubMed
-
- Croy I, Symmank A, Schellong J, Hummel C, Gerber J, Joraschky P, Hummel T. 2014. Olfaction as a marker for depression in humans. J Affect Disord. 160:80–86. - PubMed
-
- Doty RL, Shaman P, Kimmelman CP, Dann MS. 1984. University of Pennsylvania smell identification test: a rapid quantitative olfactory function test for the clinic. Laryngoscope. 94(2 Pt 1):176–178. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
