

The global burden of chronic hepatitis B virus infection: comparison of country-level prevalence estimates from four research groups
- PMID: 33367672
- PMCID: PMC8128471
- DOI: 10.1093/ije/dyaa253
The global burden of chronic hepatitis B virus infection: comparison of country-level prevalence estimates from four research groups
Abstract
Background: Progress towards viral hepatitis elimination goals relies on accurate estimates of chronic hepatitis B virus (HBV)-infection prevalence. We compared existing sources of country-level estimates from 2013 to 2017 to investigate the extent and underlying drivers of differences between them.
Methods: The four commonly cited sources of global-prevalence estimates, i.e. the Institute for Health Metrics and Evaluation, Schweitzer et al., the World Health Organization (WHO) and the CDA Foundation, were compared by calculating pairwise differences between sets of estimates and assessing their within-country variation. Differences in underlying empirical data and modelling methods were investigated as contributors to differences in sub-Saharan African estimates.
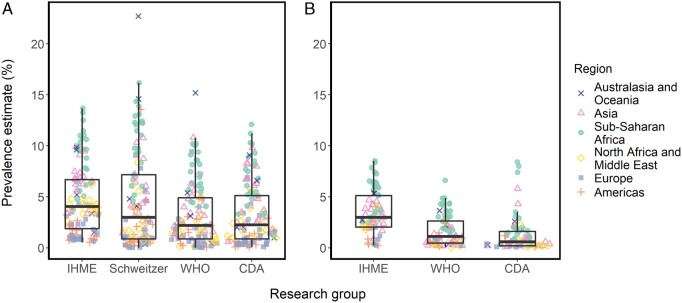
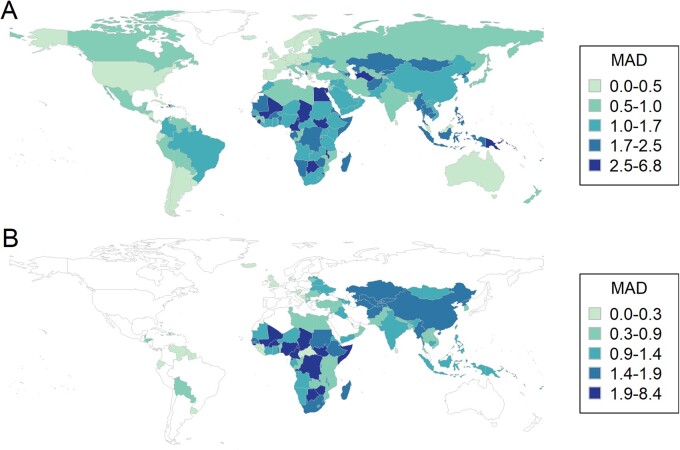
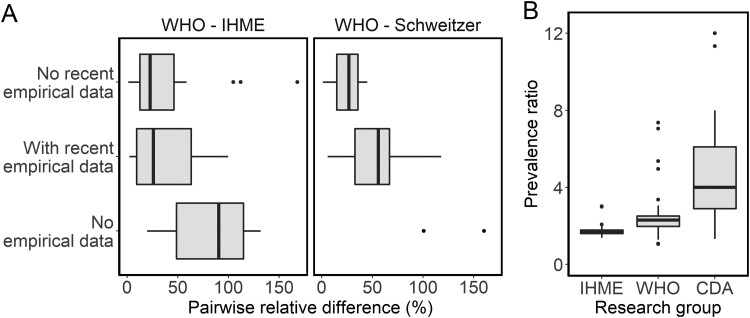
Results: The four sets of estimates across all ages were comparable overall and agreed on the global distribution of HBV burden. The WHO and the CDA produced the most similar estimates, differing by a median of 0.8 percentage points. Larger discrepancies were seen in estimates of prevalence in children under 5 years of age and in sub-Saharan African countries, where the median pairwise differences were 2.7 percentage and 2.4 percentage points for all-age prevalence and in children, respectively. Recency and representativeness of included data, and different modelling assumptions of the age distribution of HBV burden, seemed to contribute to these differences.
Conclusion: Current prevalence estimates, particularly those from the WHO and the CDA based on more recent empirical data, provide a useful resource to assess the population-level burden of chronic HBV-infection. However, further seroprevalence data in young children are needed particularly in sub-Saharan Africa. This is a priority, as monitoring progress towards elimination depends on improved knowledge of prevalence in this age group.
Keywords: Hepatitis B; disease burden; indicator; infectious diseases; modelling; monitoring; prevalence; sub-Saharan Africa; viral-hepatitis elimination.
© The Author(s) 2020. Published by Oxford University Press on behalf of the International Epidemiological Association.
Figures
References
-
- World Health Organization. WHO Global Hepatitis Report. Geneva: World Health Organization, 2017.
-
- Spearman CW, Afihene M, Ally R. et al. Hepatitis B in sub-Saharan Africa: strategies to achieve the 2030 elimination targets. Lancet Gastroenterol Hepatol 2017;2:900–09. - PubMed
-
- World Health Organization Africa. Hepatitis Scorecard for the WHO Africa Region Implementing the Hepatitis Elimination Strategy. 2019. https://www.afro.who.int/publications/hepatitis-scorecard-who-africa-reg... (1 July 2020, date last accessed).
-
- Schweitzer A, Horn J, Mikolajczyk RT, Krause G, Ott JJ.. Estimations of worldwide prevalence of chronic hepatitis B virus infection: a systematic review of data published between 1965 and 2013. Lancet 2015;386:1546–55. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
