

Intensive Care Unit-Like Care of Nonhuman Primates with Ebola Virus Disease
- PMID: 33367826
- PMCID: PMC8366444
- DOI: 10.1093/infdis/jiaa781
Intensive Care Unit-Like Care of Nonhuman Primates with Ebola Virus Disease
Abstract
Background: Ebola virus disease (EVD) supportive care strategies are largely guided by retrospective observational research. This study investigated the effect of EVD supportive care algorithms on duration of survival in a controlled nonhuman primate (NHP) model.
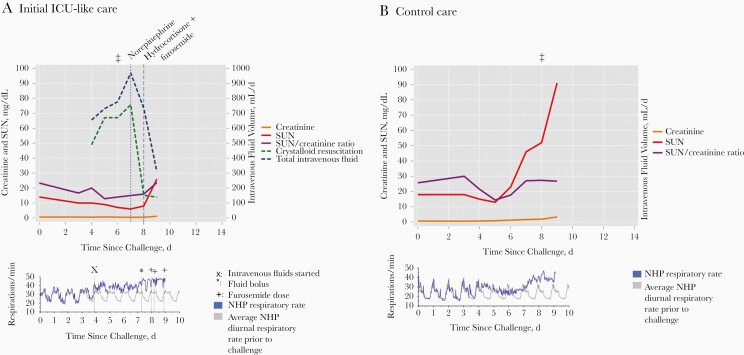
Methods: Fourteen rhesus macaques were challenged intramuscularly with a target dose of Ebola virus (1000 plaque-forming units; Kikwit). NHPs were allocated to intensive care unit (ICU)-like algorithms (n = 7), intravenous fluids plus levofloxacin (n = 2), or a control group (n = 5). The primary outcome measure was duration of survival, and secondary outcomes included changes in clinical laboratory values.
Results: Duration of survival was not significantly different between the pooled ICU-like algorithm and control groups (8.2 vs 6.9 days of survival; hazard ratio; 0.50; P = .25). Norepinephrine was effective in transiently maintaining baseline blood pressure. NHPs treated with ICU-like algorithms had delayed onset of liver and kidney injury.
Conclusions: While an obvious survival difference was not observed with ICU-like care, clinical observations from this model may aid in EVD supportive care NHP model refinement.
Keywords: Ebola virus disease; Filoviridae; Mononegavirales; animal; hemorrhagic fevers; intensive care; models; viral.
Published by Oxford University Press for the Infectious Diseases Society of America 2020.
Figures




References
-
- Lamontagne F, Clément C, Kojan R, Godin M, Kabuni P, Fowler RA. The evolution of supportive care for Ebola virus disease. Lancet 2019; 393:620–1. - PubMed
-
- Fischer WA 2nd, Crozier I, Bausch DG, et al. Shifting the paradigm—applying universal standards of care to Ebola virus disease. N Engl J Med 2019; 380:1389–91. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
