

Severe Acute Respiratory Syndrome Coronavirus 2 Serosurveillance in a Patient Population Reveals Differences in Virus Exposure and Antibody-Mediated Immunity According to Host Demography and Healthcare Setting
- PMID: 33367847
- PMCID: PMC7798933
- DOI: 10.1093/infdis/jiaa788
Severe Acute Respiratory Syndrome Coronavirus 2 Serosurveillance in a Patient Population Reveals Differences in Virus Exposure and Antibody-Mediated Immunity According to Host Demography and Healthcare Setting
Abstract
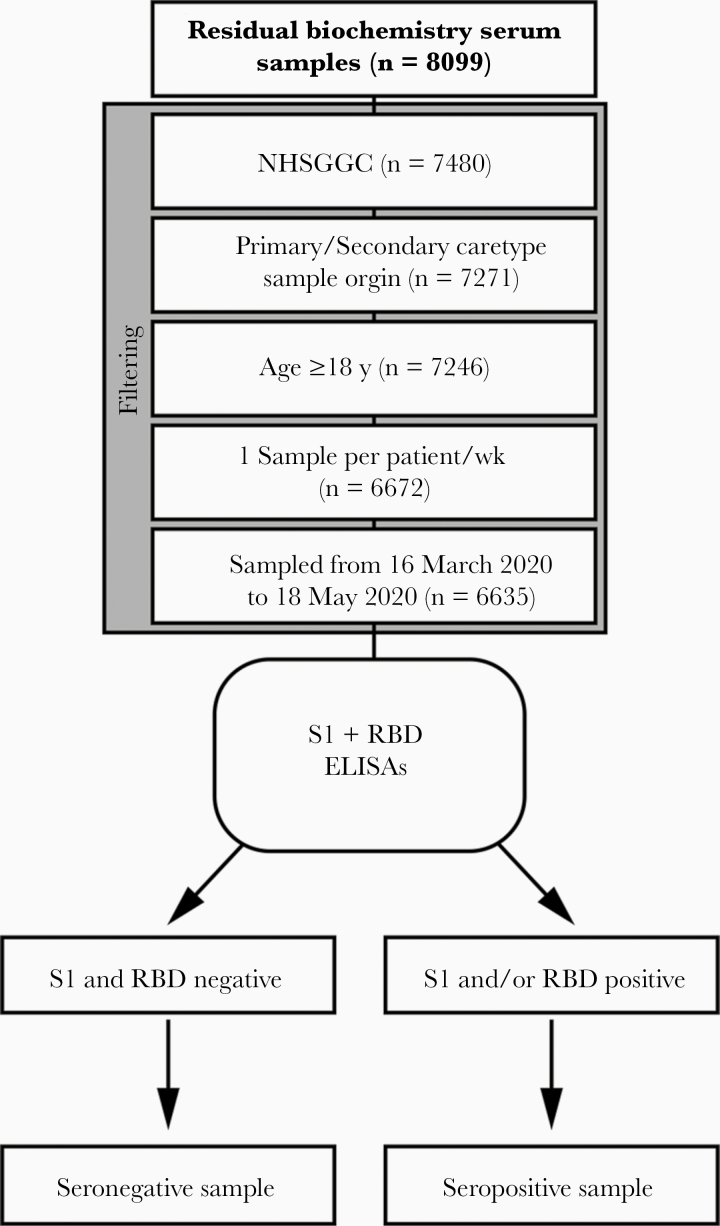
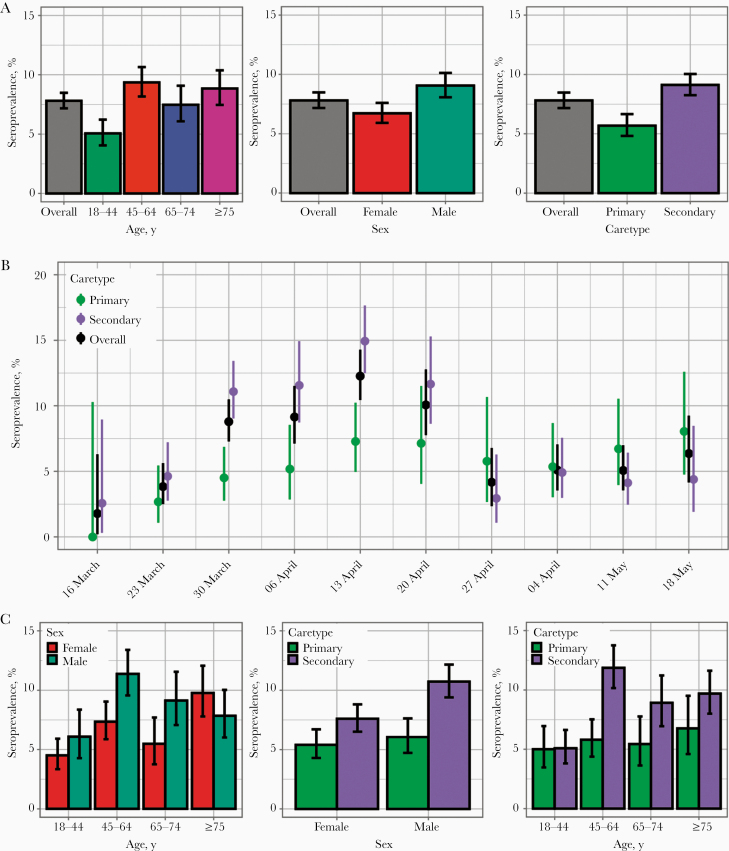
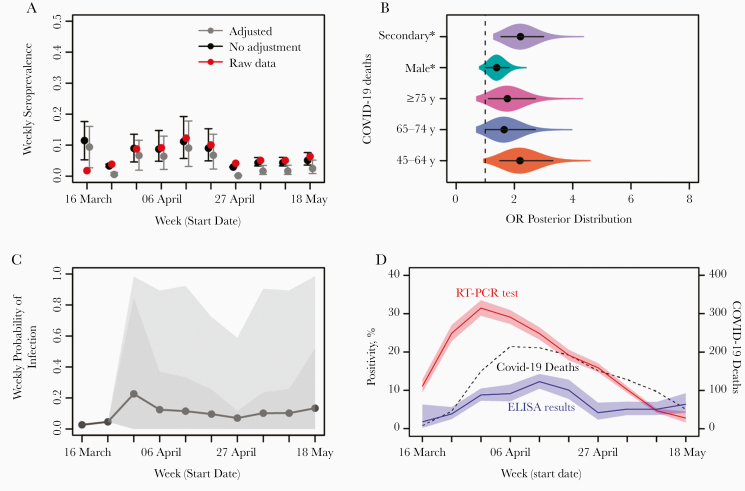
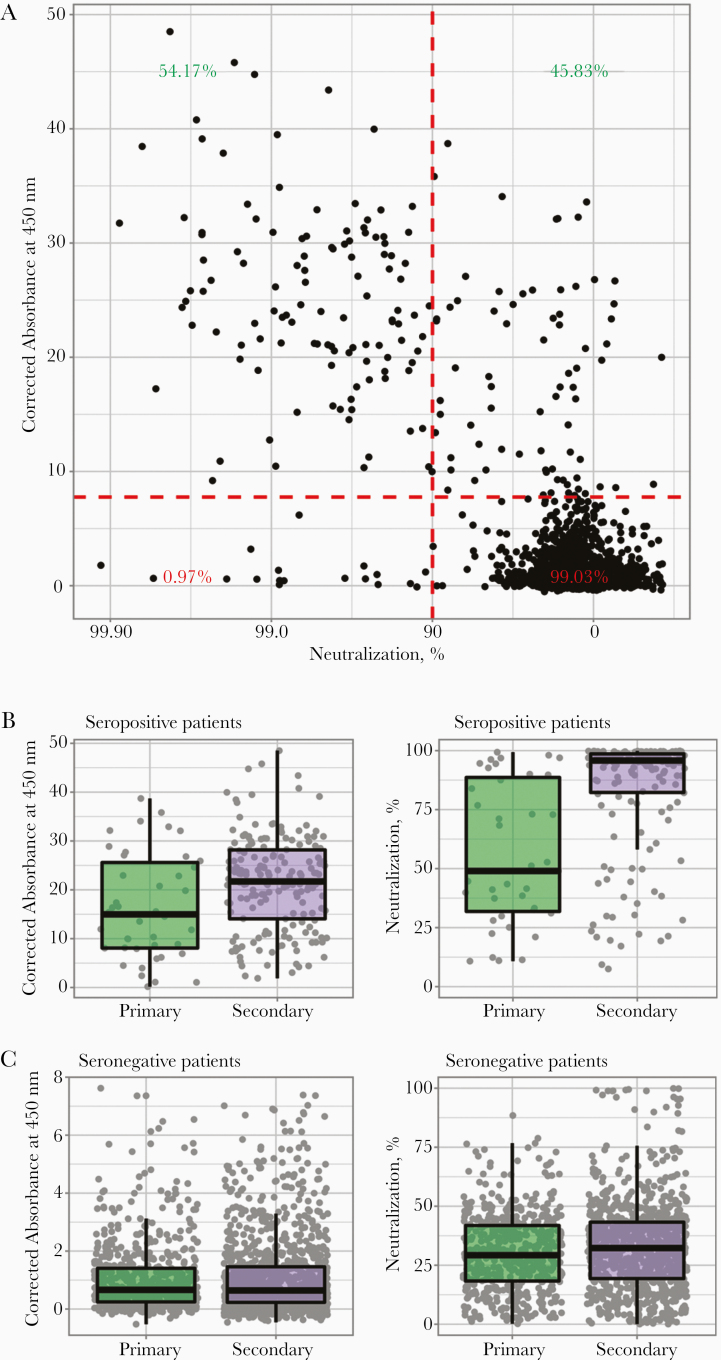
Identifying drivers of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) exposure and quantifying population immunity is crucial to prepare for future epidemics. We performed a serial cross-sectional serosurvey throughout the first pandemic wave among patients from the largest health board in Scotland. Screening of 7480 patient serum samples showed a weekly seroprevalence ranging from 0.10% to 8.23% in primary and 0.21% to 17.44% in secondary care, respectively. Neutralization assays showed that highly neutralizing antibodies developed in about half of individuals who tested positive with enzyme-linked immunosorbent assay, mainly among secondary care patients. We estimated the individual probability of SARS-CoV-2 exposure and quantified associated risk factors. We show that secondary care patients, male patients, and 45-64-year-olds exhibit a higher probability of being seropositive. The identification of risk factors and the differences in virus neutralization activity between patient populations provided insights into the patterns of virus exposure during the first pandemic wave and shed light on what to expect in future waves.
Keywords: COVID-19; SARS-CoV-2; modelling; risk factors; serology; seroprevalence; virus exposure; virus neutralization.
© The Author(s) 2020. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Coronavirus (COVID-19): Scotland’s route map. https://www.gov.scot/collections/coronavirus-covid-19-scotlands-route-map/. Accessed .
-
- World Health Organization. Establishment of the WHO International Standard and Reference Panel for anti-SARS-CoV-2 antibody. https://www.who.int/publications/m/item/WHO-BS-2020.2403. Accessed 18 November 2020.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
