

Prognostic validation and clinical implications of the EANO ESMO classification of leptomeningeal metastasis from solid tumors
- PMID: 33367859
- PMCID: PMC8301235
- DOI: 10.1093/neuonc/noaa298
Prognostic validation and clinical implications of the EANO ESMO classification of leptomeningeal metastasis from solid tumors
Erratum in
-
Erratum to: Prognostic validation and clinical implications of the EANO ESMO classification of leptomeningeal metastasis from solid tumors.Neuro Oncol. 2021 Dec 1;23(12):2126. doi: 10.1093/neuonc/noab084. Neuro Oncol. 2021. PMID: 34297825 Free PMC article. No abstract available.
Abstract
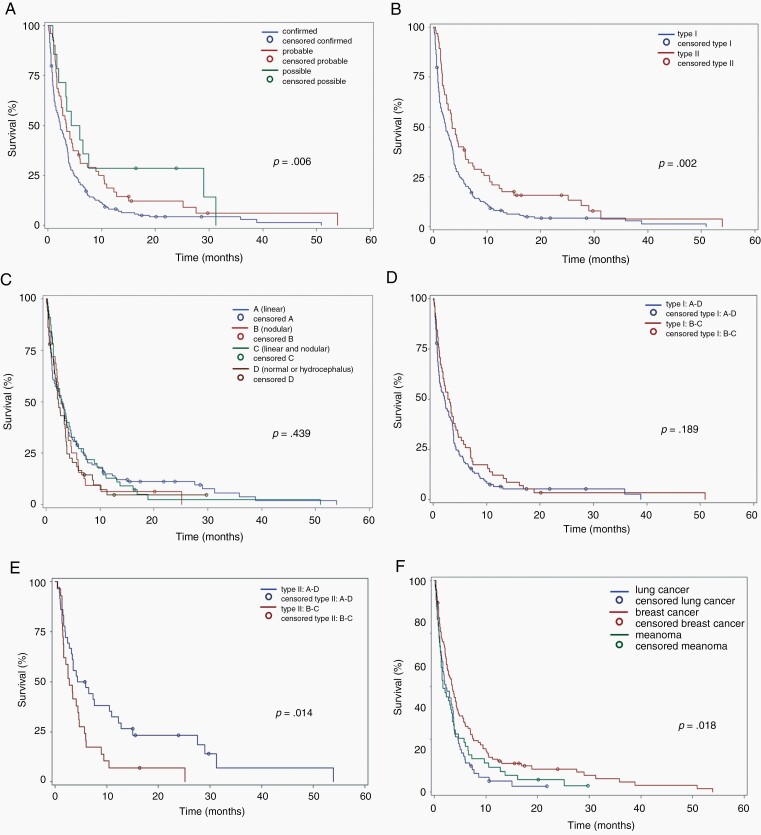
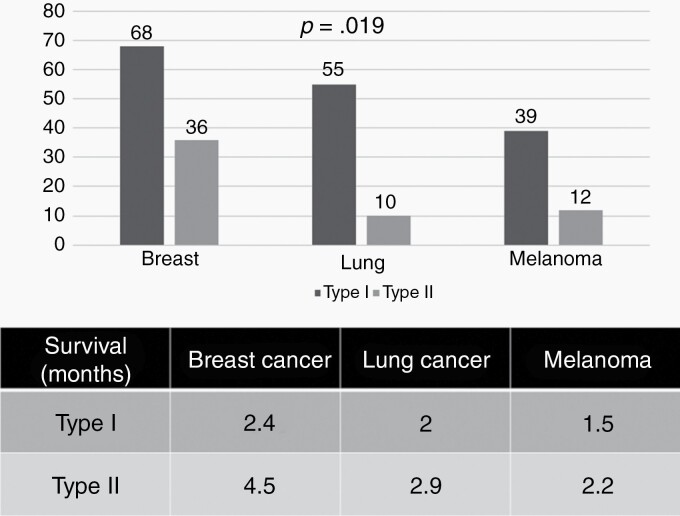
Background: The EANO ESMO guidelines have proposed a classification of leptomeningeal metastases (LM) from solid cancers based on clinical, magnetic resonance imaging (MRI), and cerebrospinal fluid (CSF) cytology presentation. MRI patterns are classified as linear, nodular, both, or neither. Type I LM is defined by positive CSF cytology (confirmed LM) whereas type II LM is defined by typical clinical and MRI signs (probable or possible LM). Here we explored the clinical utility of these LM subtypes.
Patients and methods: We retrospectively assembled data from 254 patients with newly diagnosed LM from solid tumors. Survival curves were derived using the Kaplan-Meier method and compared by Log-rank test.
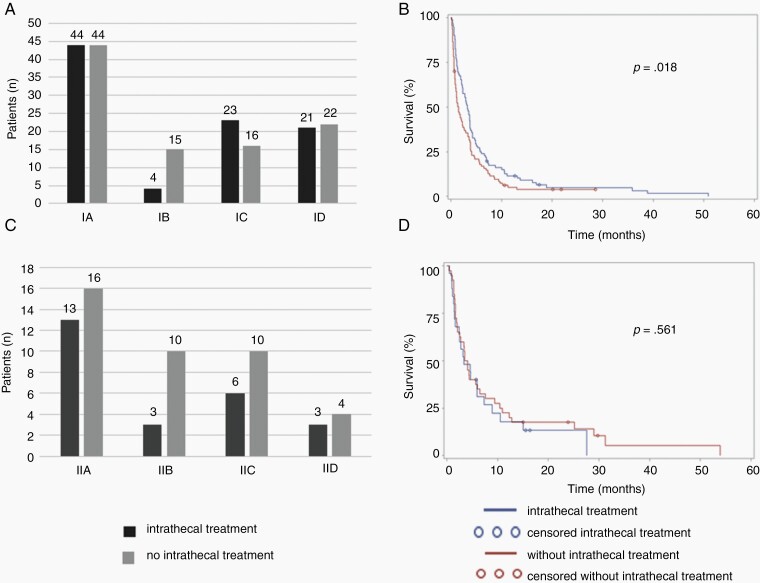
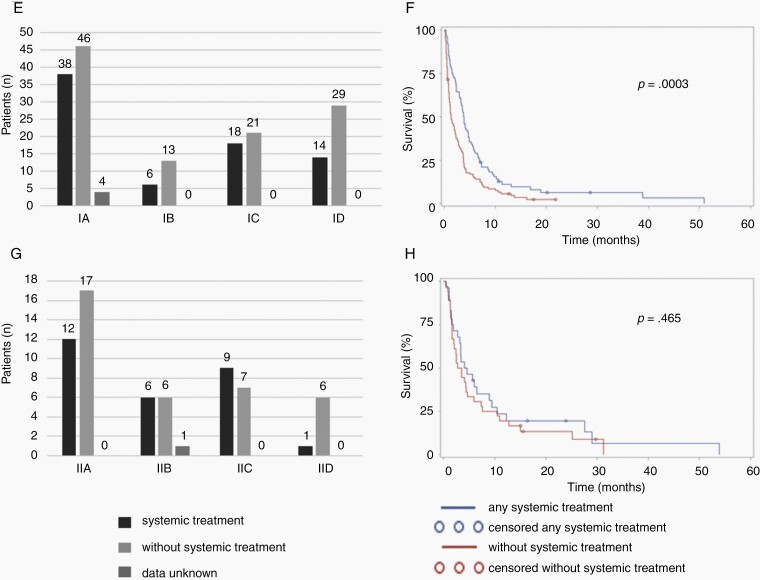
Results: Median age at LM diagnosis was 56 years. Typical clinical LM features were noted in 225 patients (89%); 13 patients (5%) were clinically asymptomatic. Tumor cells in the CSF were observed in 186 patients (73%) whereas the CSF was equivocal in 24 patients (9.5%) and negative in 44 patients (17.5%). Patients with confirmed LM had inferior outcome compared with patients with probable or possible LM (P = 0.006). Type I patients had inferior outcome than type II patients (P = 0.002). Nodular disease on MRI was a negative prognostic factor in type II LM (P = 0.014), but not in type I LM. Administration of either intrathecal pharmacotherapy (P = 0.020) or systemic pharmacotherapy (P = 0.0004) was associated with improved outcome in type I LM, but not in type II LM.
Conclusion: The EANO ESMO LM subtypes are highly prognostic and should be considered for stratification and overall design of clinical trials.
Keywords: cerebrospinal; fluid; intrathecal; meningitis; neoplastic.
© The Author(s) 2020. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
Comment in
-
Prognostic factors in leptomeningeal metastases.Neuro Oncol. 2021 Jul 1;23(7):1208-1209. doi: 10.1093/neuonc/noab051. Neuro Oncol. 2021. PMID: 33830220 Free PMC article. No abstract available.
-
The relevance of surgical status in nodular leptomeningeal metastasis patient outcomes.Neuro Oncol. 2021 Jul 1;23(7):1207. doi: 10.1093/neuonc/noab035. Neuro Oncol. 2021. PMID: 33830265 Free PMC article. No abstract available.
-
Lepto mets: loads of data.Neuro Oncol. 2021 Jul 1;23(7):1044-1045. doi: 10.1093/neuonc/noab089. Neuro Oncol. 2021. PMID: 33940636 Free PMC article. No abstract available.
References
-
- Brufsky AM, Mayer M, Rugo HS, et al. Central nervous system metastases in patients with HER2-positive metastatic breast cancer: incidence, treatment, and survival in patients from registHER. Clin Cancer Res. 2011;17(14):4834–4843. - PubMed
-
- Seute T, Leffers P, ten Velde GP, Twijnstra A. Leptomeningeal metastases from small cell lung carcinoma. Cancer. 2005;104(8):1700–1705. - PubMed
-
- Rudnicka H, Niwińska A, Murawska M. Breast cancer leptomeningeal metastasis – the role of multimodality treatment. J Neurooncol. 2007;84(1):57–62. - PubMed
-
- Gauthier H, Guilhaume MN, Bidard FC, et al. Survival of breast cancer patients with meningeal carcinomatosis. Ann Oncol. 2010;21(11):2183–2187. - PubMed
-
- Lee S, Ahn HK, Park YH, et al. Leptomeningeal metastases from breast cancer: intrinsic subtypes may affect unique clinical manifestations. Breast Cancer Res Treat. 2011;129(3):809–817. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
