

Renal Disease in Primary Sjögren's Syndrome
- PMID: 33367966
- PMCID: PMC7991017
- DOI: 10.1007/s40744-020-00264-x
Renal Disease in Primary Sjögren's Syndrome
Abstract
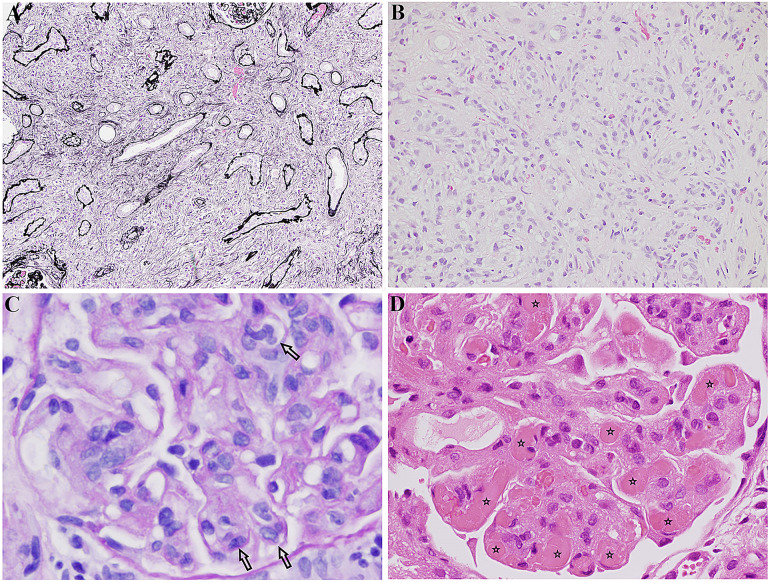
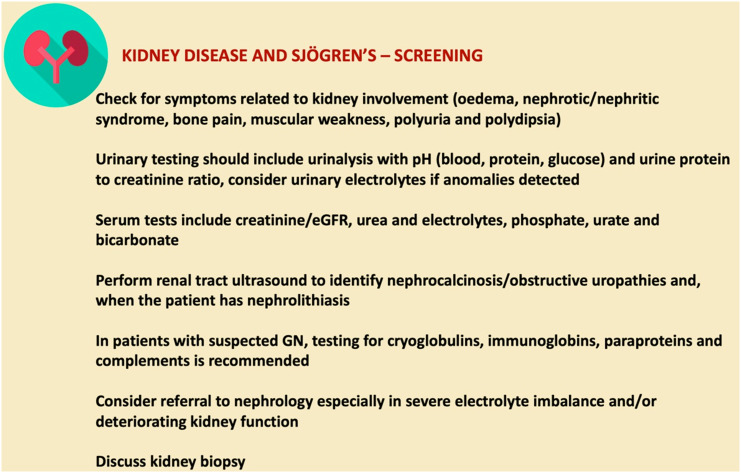
Primary Sjögren's syndrome (pSS) is a chronic autoimmune disorder characterised by lymphocytic infiltration of the exocrine glands, predominantly the salivary and lacrimal glands, leading to sicca symptoms. Patients may have extraglandular disease involving multiple organs, including the kidneys. 5% of patients with pSS can have renal involvement. Kidney disease in pSS presents a diagnostic challenge, as clinical symptoms are often insidious and can precede sicca symptoms. pSS affects the kidney through lymphocytic infiltration of renal tubules or immune complex deposition, leading to an array of clinical features. Tubulointerstitial nephritis is the most common histological pattern of kidney disease. Other tubular injuries include renal tubular acidosis with hypokalaemia, Fanconi's syndrome and diabetes insipidus. Glomerular disease is less common and typically involves an immune complex-mediated process. Optimal treatment for kidney diseases in pSS is not established, and treatment is guided by the pattern of disease. For tubulointerstitial nephritis, management involves electrolyte imbalance correction and the use of immunosuppression, including steroids. Treatment of glomerular disease is targeted to the histological pattern, and often requires a combination of immunosuppressive agents. The risk of end-stage kidney disease is low. Nevertheless, patients with pSS and kidney disease have significantly reduced quality of life.
Keywords: Glomerulonephritis; Kidney disease; Sjögren’s syndrome; Tubular dysfunction; Tubulointerstitial nephritis.
Figures
References
-
- Shiboski CH, Shiboski SC, Seror R, Criswell LA, Labetoulle M, Lietman TM, et al. 2016 American College of Rheumatology/European League Against Rheumatism classification criteria for primary Sjögren’s syndrome: a consensus and data-driven methodology involving three international patient cohorts. Arthritis Rheumatol. 2017;69(1):35–45. 10.1002/art.39859. - PMC - PubMed
-
- Baldini C, Pepe P, Quartuccio L, Priori R, Bartoloni E, Alunno A, et al. Primary Sjögren’s syndrome as a multi-organ disease: Impact of the serological profile on the clinical presentation of the disease in a large cohort of Italian patients. Rheumatol (Oxf). 2014;53(5):839–44. 10.1093/rheumatology/ket427. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
