

Automated Pupillometry Identifies Absence of Intracranial Pressure Elevation in Intracerebral Hemorrhage Patients
- PMID: 33367973
- PMCID: PMC8285349
- DOI: 10.1007/s12028-020-01146-4
Automated Pupillometry Identifies Absence of Intracranial Pressure Elevation in Intracerebral Hemorrhage Patients
Abstract
Introduction: Although automated pupillometry is increasingly used in critical care settings, predictive value of automatically assessed pupillary parameters during different intracranial pressure (ICP) levels and possible clinical implications are unestablished.
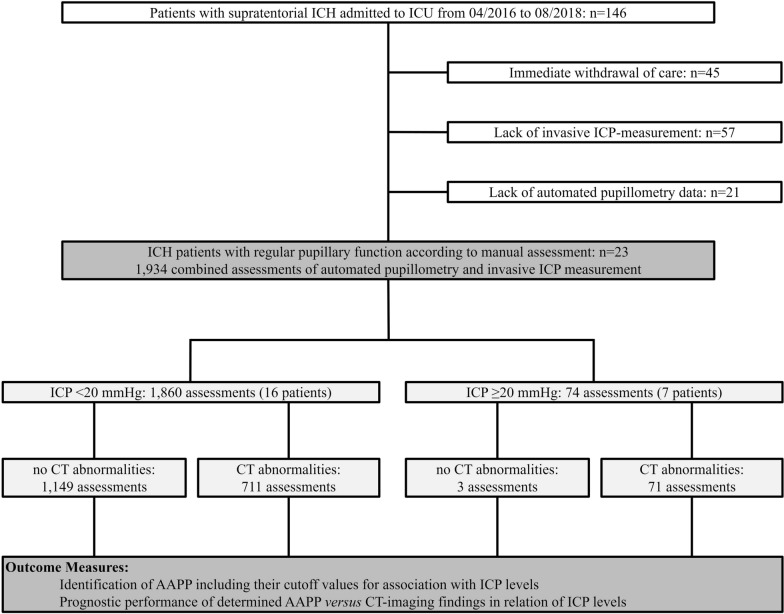
Methods: This retrospective cohort study at the neurocritical care unit of the University of Erlangen-Nuremberg (2016-2018) included 23 nontraumatic supratentorial (intracerebral hemorrhage) ICH patients without signs of abnormal pupillary function by manual assessment, i.e., absent light reflex. We assessed ICP levels by an external ventricular drain simultaneously with parameters of pupillary reactivity [i.e., maximum and minimum apertures, light reflex latency (Lat), constriction and redilation velocities (CV, DV), and percentage change of apertures (per-change)] using a portable pupillometer (NeurOptics®). Computed tomography (CT) scans were analyzed to determine lesion location, size, intraventricular hemorrhage, hydrocephalus, midline shift, and compression or absence of the basal cisterns. We performed receiver operating characteristics analysis to investigate associations of ICP levels with pupillary parameters and to determine best cutoff values for prediction of ICP elevation. After dichotomization of assessments according to ICP values (normal: < 20 mmHg, elevated: ≥ 20 mmHg), prognostic performance of the determined cutoff parameters of pupillary function versus of CT-imaging findings was analyzed by calculating sensitivity, specificity, positive and negative predictive values (logistic regression, corresponding ORs with 95% CIs).
Results: In 23 patients (11 women, median age 59.0 (51.0-69.0) years), 1,934 assessments were available for analysis. A total of 74 ICP elevations ≥ 20 mmHg occurred in seven patients. Best discriminative thresholds for ICP elevation were: CV < 0.8 mm/s (AUC 0.740), per-change < 10% (AUC 0.743), DV < 0.2 mm/s (AUC 0.703), and Lat > 0.3 s (AUC 0.616). Positive predictive value of all four parameters to indicate ICP elevation ranged between 7.2 and 8.3% only and was similarly low for CT abnormalities (9.1%). We found high negative predictive values of pupillary parameters [CV: 99.2% (95% CI 98.3-99.6), per-change: 98.7% (95% CI 97.8-99.2), DV: 98.0% (95% CI 97.0-98.7), Lat: 97.0% (95% CI 96.0-97.7)], and CT abnormalities [99.7% (95% CI 99.2-99.9)], providing evidence that both techniques adequately identified ICH patients without ICP elevation.
Conclusions: Our data suggest an association between noninvasively detected changes in pupillary reactivity and ICP levels in sedated ICH patients. Although automated pupillometry and neuroimaging seem not sufficient to noninvasively indicate ICP elevation, both techniques, however, adequately identified ICH patients without ICP elevation. This finding may facilitate routine management by saving invasive ICP monitoring or repeated CT controls in patients with specific automated pupillometry readings.
Keywords: Constriction velocity; Critical care; Intracerebral hemorrhage; Intracranial pressure; Pupillary reactivity.
© 2020. The Author(s).
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures


References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
