

Atypia of undetermined significance/follicular lesions of undetermined significance: What radiologists need to know
- PMID: 33369519
- PMCID: PMC8041409
- DOI: 10.1177/1971400920983566
Atypia of undetermined significance/follicular lesions of undetermined significance: What radiologists need to know
Abstract
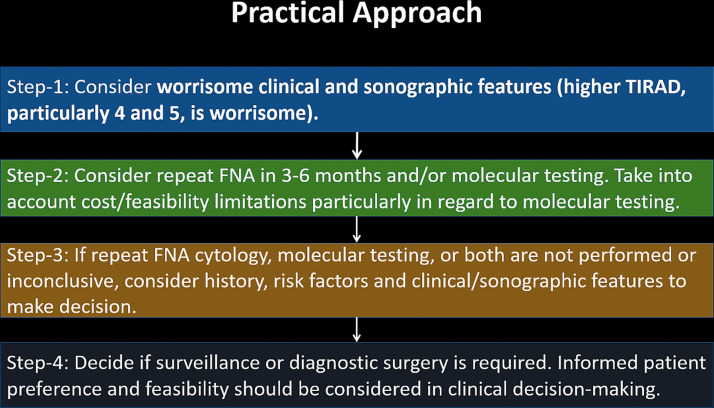
Atypia of undetermined significance/follicular lesions of undetermined significance (AUS/FLUS) refers to an intermediate histologic category of thyroid nodules in The Bethesda System for Reporting Thyroid Cytopathology. Although the risk of malignancy in this category was originally cited as 5-15%, recent literature has suggested higher rates of related malignancy ranging from 38% to 55%. Malignant nodules warrant surgery with total thyroidectomy or thyroid lobectomy, whereas benign nodules can be observed or followed with serial ultrasounds (US) based on their imaging characteristics. The management of nodules with a cytopathologic diagnosis of AUS/FLUS can be difficult because theses nodules lie between the extremes of benign and malignant. The management options for such nodules include observation, repeat fine-needle aspiration, and surgery. The use of molecular genetics, the identification of suspicious US characteristics, and the recognition of additional clinical factors are all important in the development of an appropriate, tailored management approach. Institutional factors also play a crucial role.
Keywords: Atypia of undetermined significance; Bethesda category III; Thyroid Imaging Reporting and Data System; follicular lesion of undetermined significance; thyroid nodule.
Figures
References
-
- Correa P, Chen VW. Endocrine gland cancer. Cancer 1995; 75: 338–352. - PubMed
-
- American Cancer Society. Key Statistics for Thyroid Cancer, 2020. Available at: https://cancerstatisticscenter.cancer.org/#!/cancer-site/Thyroid
-
- Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016; 26: 1–133. - PMC - PubMed
-
- Çuhaci N, Arpaci D, Üçler R, et al. Malignancy rate of thyroid nodules defined as follicular lesion of undetermined significance and atypia of undetermined significance in thyroid cytopathology and its relation with ultrasonographic features. Endocr Pathol 2014; 25: 248–256. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
