

Obtaining Quality Extended Field-of-View Ultrasound Images of Skeletal Muscle to Measure Muscle Fascicle Length
- PMID: 33369599
- PMCID: PMC8961472
- DOI: 10.3791/61765
Obtaining Quality Extended Field-of-View Ultrasound Images of Skeletal Muscle to Measure Muscle Fascicle Length
Abstract
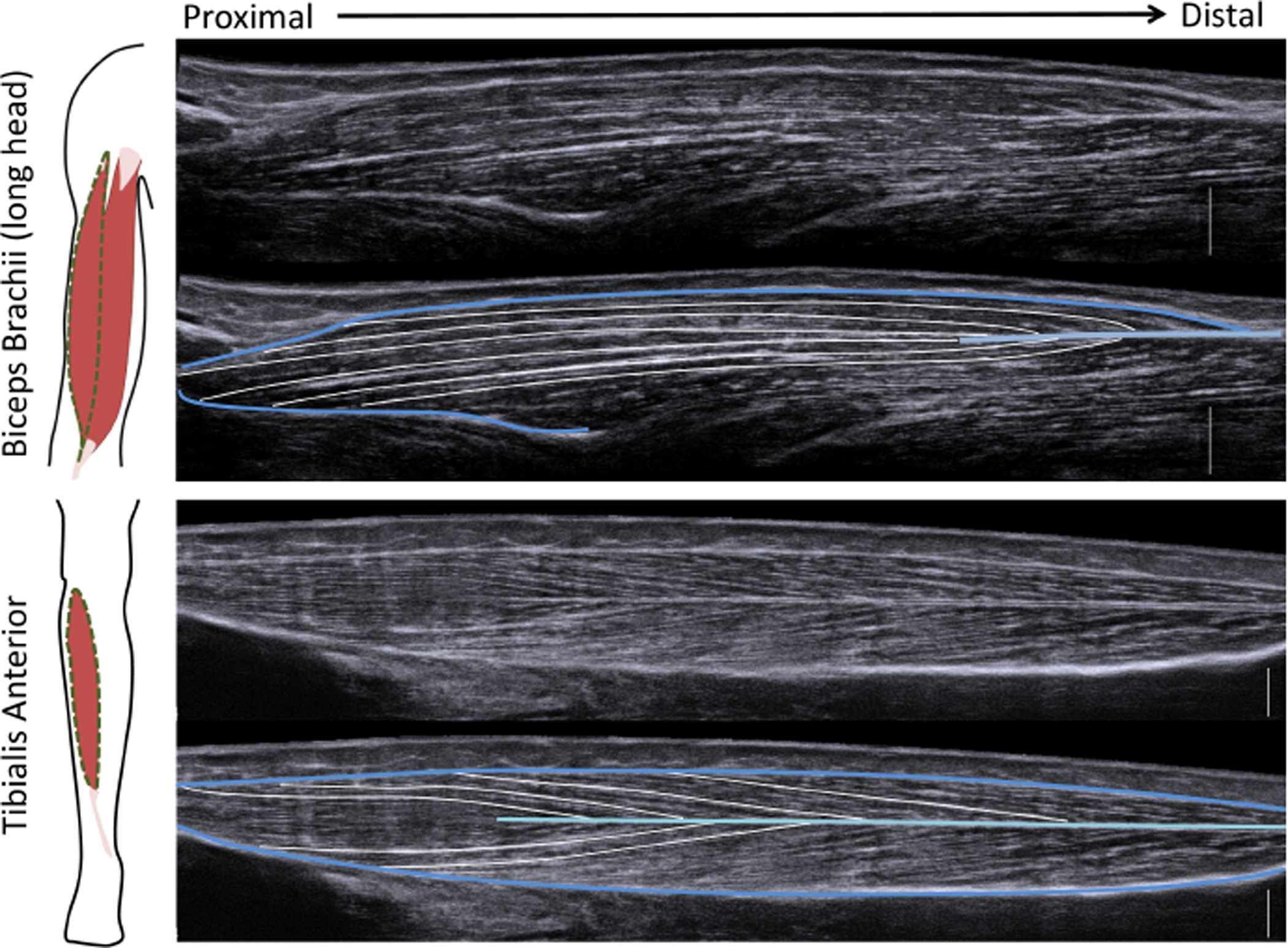
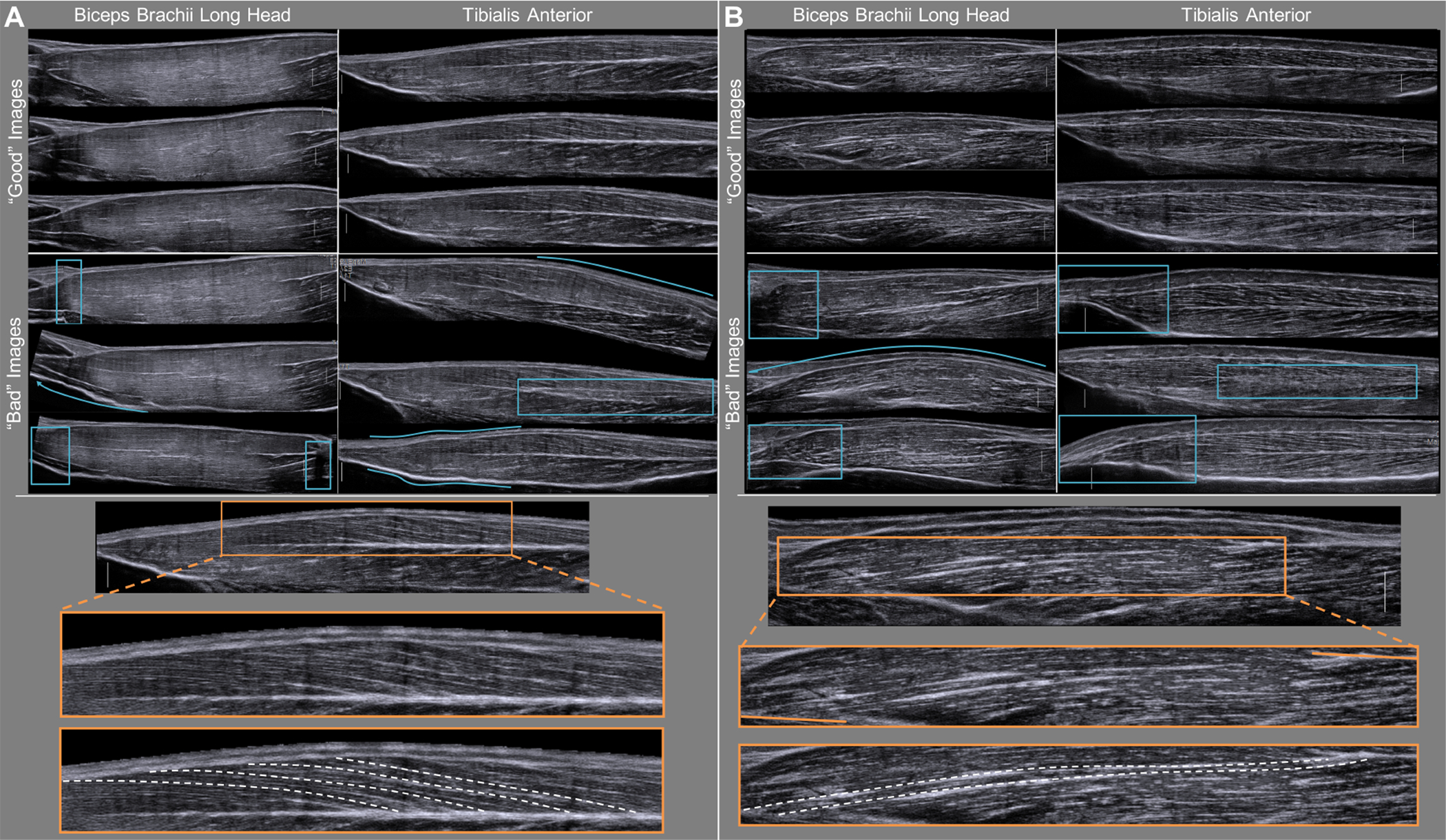
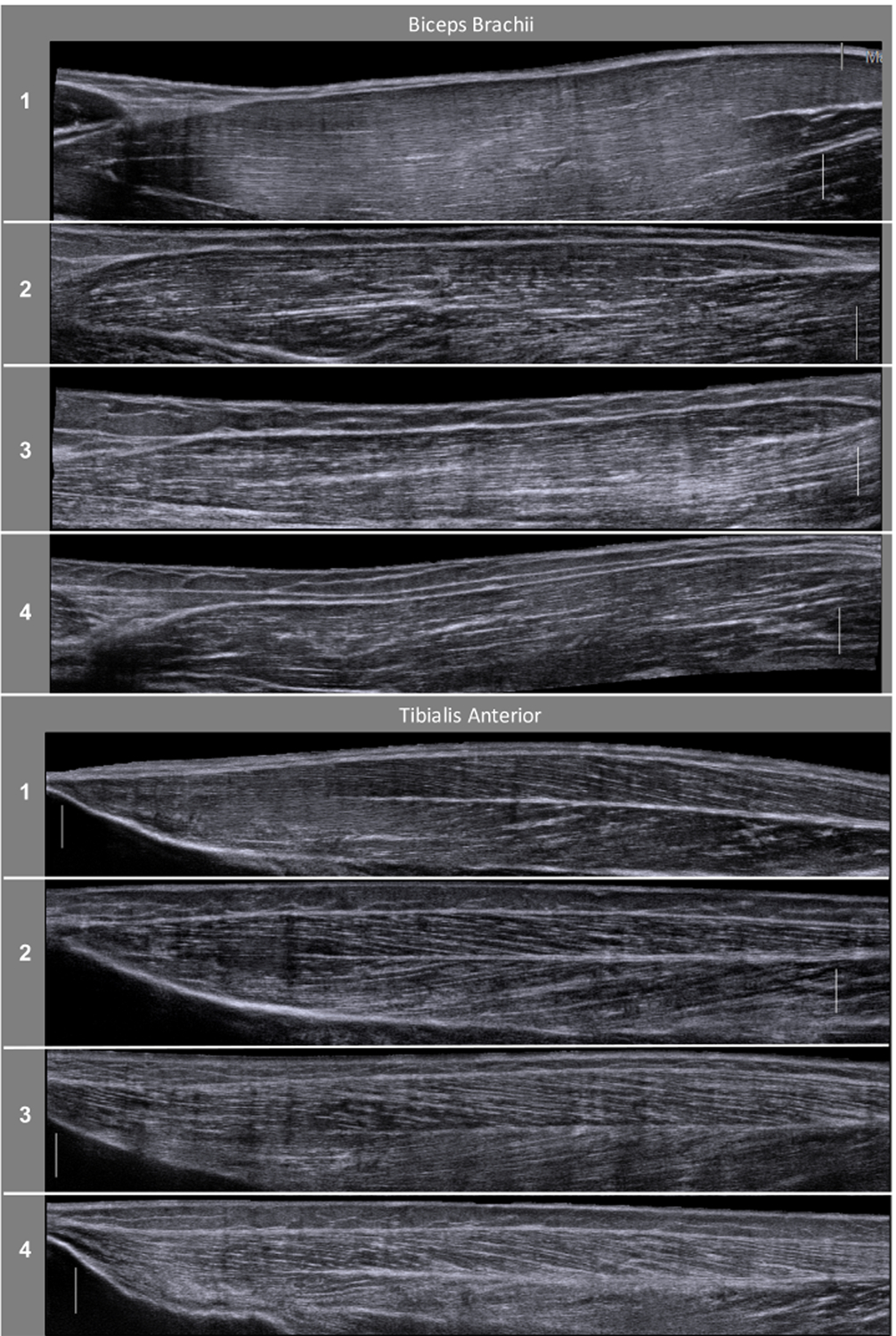
Muscle fascicle length, which is commonly measured in vivo using traditional ultrasound, is an important parameter defining a muscle's force generating capacity. However, over 90% of all upper limb muscles and 85% of all lower limb muscles have optimal fascicle lengths longer than the field-of-view of common traditional ultrasound (T-US) probes. A newer, less frequently adopted method called extended field-of-view ultrasound (EFOV-US) can enable direct measurement of fascicles longer than the field-of-view of a single T-US image. This method, which automatically fits together a sequence of T-US images from a dynamic scan, has been demonstrated to be valid and reliable for obtaining muscle fascicle lengths in vivo. Despite the numerous skeletal muscles with long fascicles and the validity of the EFOV-US method for making measurements of such fascicles, few published studies have utilized this method. In this study, we demonstrate both how to implement the EFOV-US method to obtain high quality musculoskeletal images and how to quantify fascicle lengths from those images. We expect that this demonstration will encourage the use of the EFOV-US method to increase the pool of muscles, both in healthy and impaired populations, for which we have in vivo muscle fascicle length data.
Figures
References
-
- Gans C & Bock WJ The functional significance of muscle architecture: a theoretical analysis. Adv Anat Embryol Cell Biol. 38 115–142, (1965). - PubMed
-
- Gans C Fiber architecture and muscle function. Exercise and Sports Sciences Reviews. 10 160–207, (1982). - PubMed
-
- Lieber RL & Fridén J Functional and clinical significance of skeletal muscle architecture. Muscle & Nerve: Official Journal of the American Association of Electrodiagnostic Medicine. 23 (11), 1647–1666, (2000). - PubMed
-
- Zajac FE Muscle and tendon: properties, models, scaling, and application to biomechanics and motor control. Critical reviews in biomedical engineering. 17 (4), 359–411, (1989). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
