

The Impact of Biopsy Tool Choice and Rapid On-Site Evaluation on Diagnostic Accuracy for Malignant Lesions in the Prospective: Multicenter NAVIGATE Study
- PMID: 33369988
- PMCID: PMC8219084
- DOI: 10.1097/LBR.0000000000000740
The Impact of Biopsy Tool Choice and Rapid On-Site Evaluation on Diagnostic Accuracy for Malignant Lesions in the Prospective: Multicenter NAVIGATE Study
Abstract
Background: The diagnostic yield of electromagnetic navigation bronchoscopy (ENB) is impacted by biopsy tool strategy and rapid on-site evaluation (ROSE) use. This analysis evaluates usage patterns, accuracy, and safety of tool strategy and ROSE in a multicenter study.
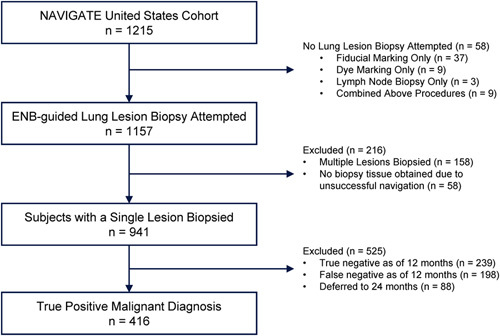
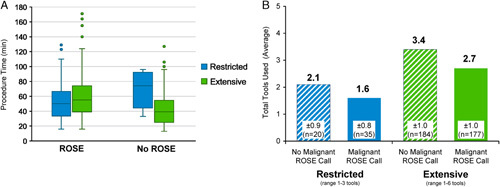
Methods: NAVIGATE (NCT02410837) evaluates ENB using the superDimension navigation system (versions 6.3 to 7.1). The 1-year analysis included 1215 prospectively enrolled subjects at 29 United States sites. Included herein are 416 subjects who underwent ENB-aided biopsy of a single lung lesion positive for malignancy at 1 year. Use of a restricted number of tools (only biopsy forceps, standard cytology brush, and/or bronchoalveolar lavage) was compared with an extensive multimodal strategy (biopsy forceps, cytology brush, aspirating needle, triple needle cytology brush, needle-tipped cytology brush, core biopsy system, and bronchoalveolar lavage).
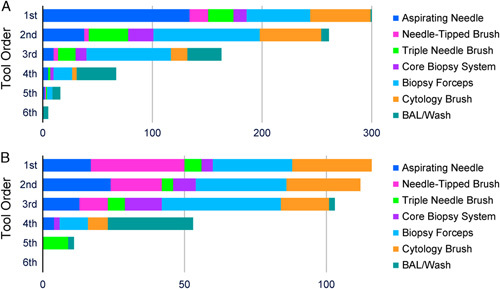
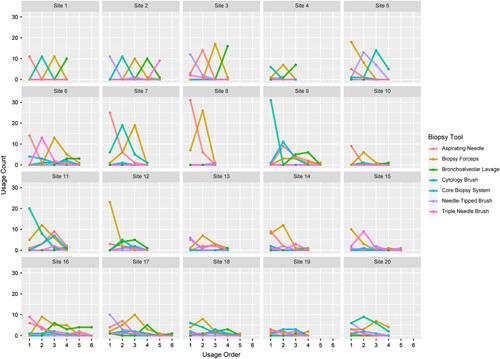
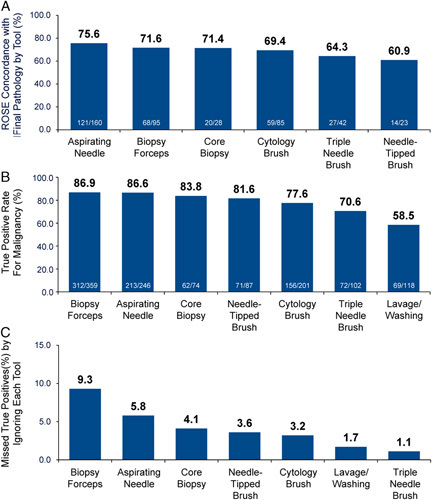
Results: Of malignant cases, 86.8% (361/416) of true positive diagnoses were obtained using extensive multimodal strategies. ROSE was used in 300/416 cases. The finding of malignancy by ROSE reduced the total number of tools used. A malignant ROSE call was obtained in 71% (212/300), most (88.7%; 188/212) by the first tool used (49.5% with aspirating needle, 20.2% with cytology brush, 17.0% with forceps). True positive rates were highest for the biopsy forceps (86.9%) and aspirating needle (86.6%). Use of extensive tool strategies did not increase the rates of pneumothorax (5.5% restricted, 2.8% extensive) or bronchopulmonary hemorrhage (3.6% restricted, 1.1% extensive).
Conclusion: These results suggest that extensive biopsy tool strategies, including the aspirating needle, may provide higher true positive rates for detecting lung cancer without increasing complications.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
Disclosure: Dr E.E.F. reports consultant fees from Medtronic and Boston Scientific, and a research grant from Intuitive Surgical. Dr T.R.G. reports travel funds from Medtronic. Dr S.J.K. reports consultant fees from Medtronic. Dr G.P.L. reports consultant fees from Medtronic. H.L. and Dr J.S.M. are full-time employees of Medtronic. Dr A.K.M. reports consultant fees from Medtronic. Dr M.A.P. reports speaking, consulting, or research payments from Medtronic, Auris Health, BodyVision, Intuitive Surgical, Philips, Biodesix, AstraZeneca, Johnson and Johnson, Boehringer Ingelheim, United Therapeutics, Actelion, Inivata, and Boston Scientific. Dr O.B.R. reports consultant fees from Medtronic. Dr J.S. reports consultant fees from Somnoware Sleep Solutions. For the remaining authors there is no conflict of interest or other disclosures.
Figures
References
-
- Gex G, Pralong JA, Combescure C, et al. . Diagnostic yield and safety of electromagnetic navigation bronchoscopy for lung nodules: a systematic review and meta-analysis. Respiration. 2014;87:165–176. - PubMed
-
- McGuire AL, Myers R, Grant K, et al. . The diagnostic accuracy and sensitivity for malignancy of radial-endobronchial ultrasound and electromagnetic navigation bronchoscopy for sampling of peripheral pulmonary lesions: systematic review and meta-analysis. J Bronchology Interv Pulmonol. 2020;27:106–121. - PubMed
-
- Folch EE, Labarca G, Ospina-Delgado D, et al. . Sensitivity and safety of electromagnetic navigation bronchoscopy for lung cancer diagnosis: systematic review and meta-analysis. Chest. 2020;158:1753–1769. - PubMed
-
- Mehta AC, Hood KL, Schwarz Y, et al. . The evolutional history of electromagnetic navigation bronchoscopy: state of the art. Chest. 2018;154:935–947. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
