

PROSPECT guideline for elective caesarean section: updated systematic review and procedure-specific postoperative pain management recommendations
- PMID: 33370462
- PMCID: PMC8048441
- DOI: 10.1111/anae.15339
PROSPECT guideline for elective caesarean section: updated systematic review and procedure-specific postoperative pain management recommendations
Abstract
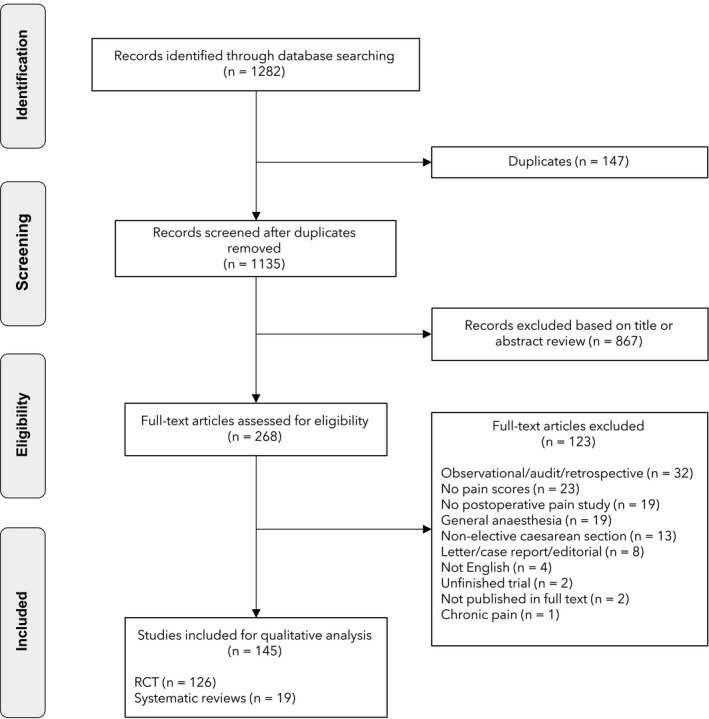
Caesarean section is associated with moderate-to-severe postoperative pain, which can influence postoperative recovery and patient satisfaction as well as breastfeeding success and mother-child bonding. The aim of this systematic review was to update the available literature and develop recommendations for optimal pain management after elective caesarean section under neuraxial anaesthesia. A systematic review utilising procedure-specific postoperative pain management (PROSPECT) methodology was undertaken. Randomised controlled trials published in the English language between 1 May 2014 and 22 October 2020 evaluating the effects of analgesic, anaesthetic and surgical interventions were retrieved from MEDLINE, Embase and Cochrane databases. Studies evaluating pain management for emergency or unplanned operative deliveries or caesarean section performed under general anaesthesia were excluded. A total of 145 studies met the inclusion criteria. For patients undergoing elective caesarean section performed under neuraxial anaesthesia, recommendations include intrathecal morphine 50-100 µg or diamorphine 300 µg administered pre-operatively; paracetamol; non-steroidal anti-inflammatory drugs; and intravenous dexamethasone administered after delivery. If intrathecal opioid was not administered, single-injection local anaesthetic wound infiltration; continuous wound local anaesthetic infusion; and/or fascial plane blocks such as transversus abdominis plane or quadratus lumborum blocks are recommended. The postoperative regimen should include regular paracetamol and non-steroidal anti-inflammatory drugs with opioids used for rescue. The surgical technique should include a Joel-Cohen incision; non-closure of the peritoneum; and abdominal binders. Transcutaneous electrical nerve stimulation could be used as analgesic adjunct. Some of the interventions, although effective, carry risks, and consequentially were omitted from the recommendations. Some interventions were not recommended due to insufficient, inconsistent or lack of evidence. Of note, these recommendations may not be applicable to unplanned deliveries or caesarean section performed under general anaesthesia.
Keywords: analgesia; caesarean delivery; caesarean section; pain.
© 2020 The Authors. Anaesthesia published by John Wiley & Sons Ltd on behalf of Association of Anaesthetists.
Figures
Comment in
-
PROSPECT guideline for elective caesarean section and the administration of dexamethasone.Anaesthesia. 2021 Sep;76(9):1278-1279. doi: 10.1111/anae.15484. Epub 2021 Apr 15. Anaesthesia. 2021. PMID: 33858031 No abstract available.
-
PROSPECT guideline for elective caesarean section.Anaesthesia. 2022 May;77(5):616. doi: 10.1111/anae.15655. Epub 2021 Dec 26. Anaesthesia. 2022. PMID: 34957552 No abstract available.
-
PROSPECT guideline for elective caesarean section: an update.Anaesthesia. 2023 Sep;78(9):1170-1171. doi: 10.1111/anae.16034. Epub 2023 Apr 27. Anaesthesia. 2023. PMID: 37104085 No abstract available.
References
-
- Gamez BH, Habib AS. Predicting severity of acute pain after Cesarean delivery: a narrative review. Anesthesia and Analgesia 2018; 126: 1606–14. - PubMed
-
- Kainu JP, Sarvela J, Tiippana E, Halmesmaki E, Korttila KT. Persistent pain after caesarean section and vaginal birth: a cohort study. International Journal of Obstetric Anesthesia 2010; 19: 4–9. - PubMed
-
- PROSPECT . Recommendations for postoperative analgesia after caesarean section 2014. www.postoppain.org (accessed 04/11/2020).
-
- Huang J, Cao C, Nelson G, Wilson RD. A review of enhanced recovery after surgery principles used for scheduled Caesarean delivery. Journal of Obstetrics and Gynecology 2019; 41: 1775–88. - PubMed
-
- Joshi GP, Schug SA, Kehlet H. Procedure‐specific pain management and outcome strategies. Best Practice and Research Clinical Anaesthesiology. 2014; 28: 191–201. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
