

Comparison of cardiovascular disease risk factors, assessment and management in men and women, including consideration of absolute risk: a nationally representative cross-sectional study
- PMID: 33371018
- PMCID: PMC7757475
- DOI: 10.1136/bmjopen-2020-038761
Comparison of cardiovascular disease risk factors, assessment and management in men and women, including consideration of absolute risk: a nationally representative cross-sectional study
Abstract
Objectives: Cardiovascular disease (CVD) is highly preventable and optimal treatments based on absolute risk can halve risk of future events. Compared with women, men have higher risks of developing CVD. However, women can experience suboptimal treatment. We aimed to quantify sex differences in CVD risk, assessment and treatment in Australian adults.
Design, participants, setting: Cross-sectional analysis of nationally representative data from interview, physical measures, medication review and blood and urine samples, from 2011 to 2012 Australian Health Survey participants aged 45-74 (n=11 518).
Outcome measures: CVD risk factors, absolute 5-year risk of a primary CVD event, blood pressure and cholesterol assessment in the previous 2 and 5 years and use of recommended CVD preventive medications were compared using Poisson regression to estimate age-adjusted male versus female prevalence ratios (PRs).
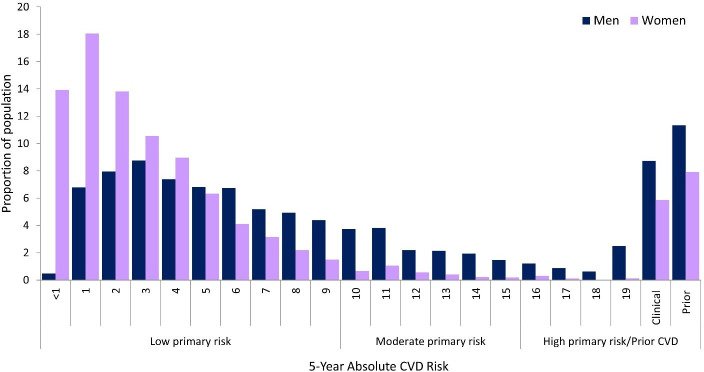
Results: Women had a generally more favourable CVD risk factor profile than men, including lower: current smoking prevalence (women=14.5%; men=18.4%, PR=0.78, 95% CI=0.70 to 0.88); body mass index (women (mean)=28.3 kg/m2; men (mean)=28.8 kg/m2, p<0.01); systolic and diastolic blood pressure (systolic: women (mean)=127.1 mm Hg; men (mean)=130.5 mm Hg, p<0.001); blood glucose (women (mean)=5.2 mmol/L; men (mean)=5.5 mmol/L); diabetes prevalence (women=6.8%; men=12.5%, PR=0.55, 95% CI=0.44 to 0.67); prior CVD (women=7.9%; men=11.3%) and absolute primary CVD risk (absolute 5-year CVD risk >15%: women=6.6%, 95% CI=5.4 to 7.8; men=15.4%, 95% CI=13.9% to 16.9%). Compared with men, women had higher low-density lipoprotein, high-density lipoprotein and total cholesterol and sedentary behaviour and lower physical activity. Blood pressure and cholesterol assessment were common in both sexes. Among those at high absolute risk, age-adjusted proportions receiving recommended CVD medications were low, without sex differences (women=21.3%; men=23.8%, PR=0.93, 95% CI=0.49 to 1.78). Fewer women than men with prior atherosclerotic CVD were receiving recommended treatment (women=21.8%, men=41.4%, PR=0.55, 95% CI=0.31 to 0.96).
Conclusion: Women have a more favourable CVD risk factor profile than men. Preventive treatment is uncommon and women with prior atherosclerotic CVD are around half as likely as men to be receiving recommended treatment.
Keywords: coronary heart disease; epidemiology; public health.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures



References
-
- Kyu HH, Abate D, Abate KH, et al. . Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. The Lancet 2018;392:1859–922. 10.1016/S0140-6736(18)32335-3 - DOI - PMC - PubMed
-
- Foreman KJ, Marquez N, Dolgert A. Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death: reference and alternative scenarios for 2016–40 for 195 countries and territories. The Lancet 2018;392:2052–90. 10.1016/S0140-6736(18)31694-5 - DOI - PMC - PubMed
-
- Australian Institute of Health and Welfare Cardiovascular disease snapshot. Canberra: AIHW, 2018.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials