

The Association between Nonalcoholic Fatty Liver Disease and Stroke: Results from the Korean Genome and Epidemiology Study (KoGES)
- PMID: 33371282
- PMCID: PMC7765788
- DOI: 10.3390/ijerph17249568
The Association between Nonalcoholic Fatty Liver Disease and Stroke: Results from the Korean Genome and Epidemiology Study (KoGES)
Abstract
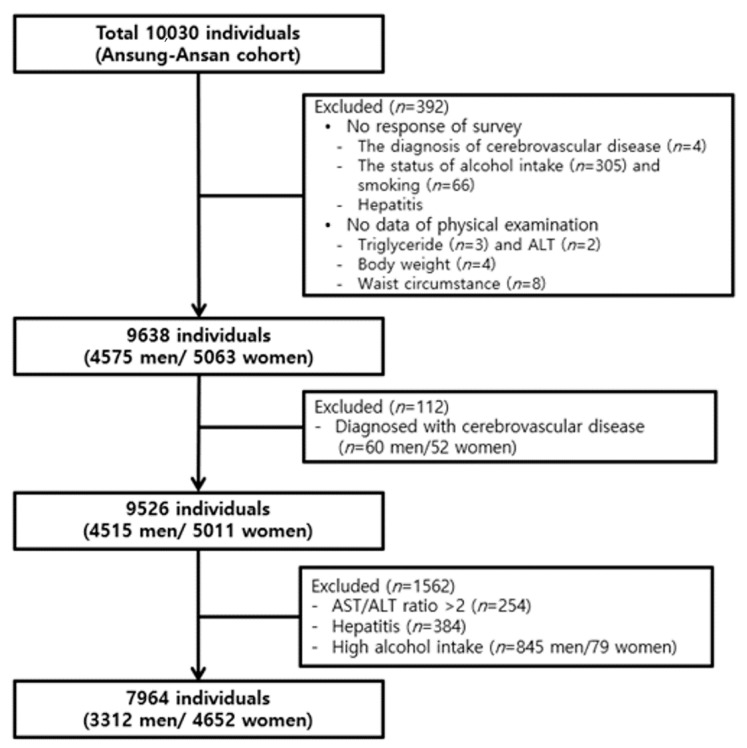
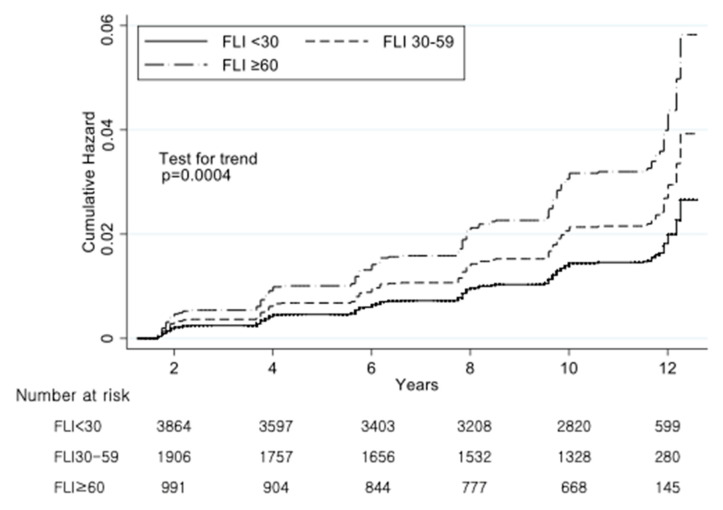
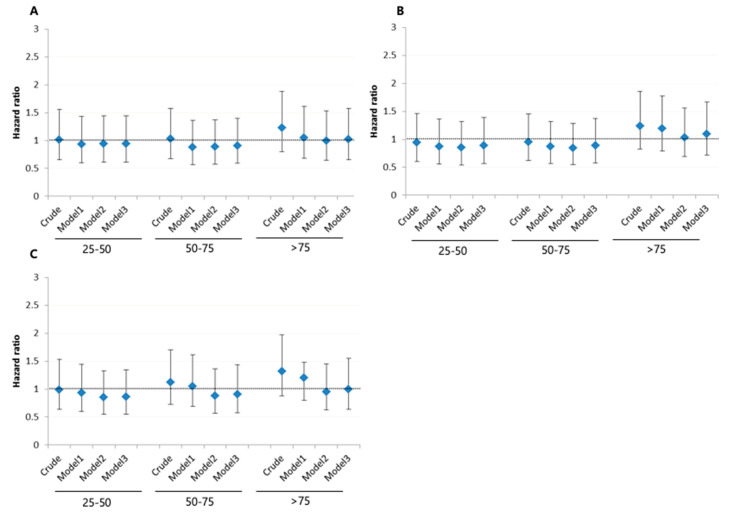
(1) Background: Non-alcoholic fatty liver disease (NAFLD) is associated with various cardiometabolic diseases. However, the association between NAFLD and stroke is not well known. The purpose of our study is to reveal the relationship between NAFLD and Stroke incidence. (2) Methods: Using data from a Korean prospective cohort study, we excluded participants with heavy alcohol consumption and a history of stroke; hence, 7964 adults aged 40-69 years were included in this study. According to their fatty liver index (FLI), participants were divided into three groups: <30 (n = 4550, non-NAFLD), 30-59.9 (n = 2229, intermediate), and ≥60 (n = 1185, NAFLD). The incidence of stroke according to the degree of FLI was evaluated using the Cox proportional hazard model. (3) Results: During the 12-year follow-up period, 168 strokes occurred. A graded association between NAFLD and stroke incidence was observed, i.e., 1.7% (n = 76), 2.5% (n = 56), and 3.0% (n = 36) for non-NAFLD, intermediate, and NAFLD FLI groups, respectively. After adjusting for confounding variables and compared to the risk of stroke in the non-NAFLD group, the risk of stroke in the NAFLD group was the highest (hazard ratio [HR]: 1.98, 95% confidence interval [CI]: 1.17-3.34), followed by the risk of stroke in the intermediate group (HR: 1.41, 95% CI: 0.94-2.21) (p for trend < 0.001). However, the level of aspartate aminotransferase, alanine aminotransferase, or gamma-glutamyltransferase alone did not show any significant association with stroke. (4) Conclusions: This study demonstrated that the risk of stroke incidence gradually increased with the degree of FLI. Individuals with NAFLD should be properly counseled and monitored for risk for stroke.
Keywords: cohort studies; incidence; liver; non-alcoholic fatty liver disease; risk factors; stroke.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Benjamin E.J., Blaha M.J., Chiuve S.E., Cushman M., Das S.R., Deo R., de Ferranti S.D., Floyd J., Fornage M., Gillespie C., et al. Heart Disease and Stroke Statistics-2017 Update: A Report From the American Heart Association. Circulation. 2017;135:e146–e603. doi: 10.1161/CIR.0000000000000485. - DOI - PMC - PubMed
-
- Feigin V.L., Roth G.A., Naghavi M., Parmar P., Krishnamurthi R., Chugh S., Mensah G.A., Norrving B., Shiue I., Ng M., et al. Global burden of stroke and risk factors in 188 countries, during 1990–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet Neurol. 2016;15:913–924. doi: 10.1016/S1474-4422(16)30073-4. - DOI - PubMed
-
- Hong K.S., Bang O.Y., Kang D.W., Yu K.H., Bae H.J., Lee J.S., Heo J.H., Kwon S.U., Oh C.W., Lee B.C., et al. Stroke statistics in Korea: Part I. Epidemiology and risk factors: A report from the korean stroke society and clinical research center for stroke. J. Stroke. 2013;15:2–20. doi: 10.5853/jos.2013.15.1.2. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
