

Clinical governance programme in patients with acute coronary syndrome: design and methodology of a quality improvement initiative
- PMID: 33372102
- PMCID: PMC7768950
- DOI: 10.1136/openhrt-2020-001415
Clinical governance programme in patients with acute coronary syndrome: design and methodology of a quality improvement initiative
Abstract
Introduction: Despite the availability of diverse evidence-based diagnostic and treatment options, many patients with acute coronary syndrome (ACS) still fail to receive effective, safe and timely diagnoses and therapies. The Association of Acute CardioVascular Care of the European Society of Cardiology has proposed and retrospectively validated a set of ACS-specific quality indicators. Combining these indicators with the principles of clinical governance-a holistic, patient-centred approach intended to promote continuous quality improvement-we designed the clinical governance programme in patients with ACS.
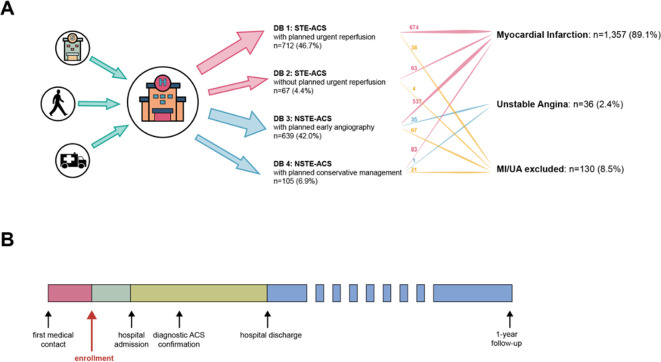
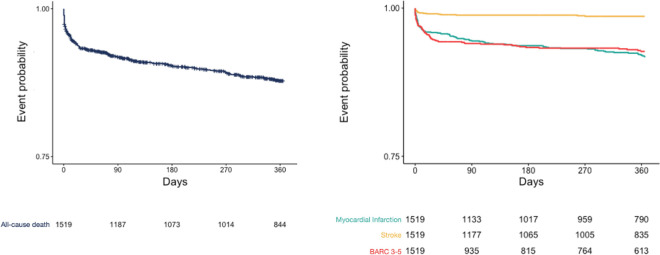
Methods and analysis: This is a multicentre quality improvement initiative exploring multiple dimensions of care, including diagnosis, therapy, patient satisfaction, centre organisation and efficiency in all comers patients with ACS.The study will enrol ≈ 5000 patients prospectively (ie, at the time of the first objective qualifying ACS criterion) with a 1-year follow-up. Consecutive inclusion will be promoted by a simplified informed consent process and quantified by the concordance with corresponding hospital administrative records using diagnosis-related group codes of ACS.Coprimary outcome measures are (1) timely reperfusion in patients with ST-elevation ACS and (2) optimal medical therapy at discharge in patients with confirmed acute myocardial infarction. Secondary outcomes broadly include multiple indicators of the process of care. Clinical endpoints (ie, death, myocardial infarction, stroke and bleeding) will be adjudicated by a clinical event committee according to predefined criteria.
Ethics and dissemination: The study has been approved by local ethics committee of all study sites. As a quality improvement initiative and to promote consecutive inclusion of the population of interest, a written informed consent will be requested only to patients who are discharged alive. Dissemination will be actively promoted by (1) the registration site (ClinicalTrials.Gov ID NCT04255537), (2) collaborations with investigators through open data access and sharing.
Keywords: acute coronary syndrome; myocardial ischaemia and infarction (IHD); quality of care and outcomes.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: SL reports personal fees for advisory board participation from AstraZeneca, Chiesi, BMS/Pfizer, Novo Nordisk, and The Medicine Company, outside the submitted work.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials