

Presence of the neonatal Staphylococcus capitis outbreak clone (NRCS-A) in prosthetic joint infections
- PMID: 33372186
- PMCID: PMC7769963
- DOI: 10.1038/s41598-020-79225-x
Presence of the neonatal Staphylococcus capitis outbreak clone (NRCS-A) in prosthetic joint infections
Abstract
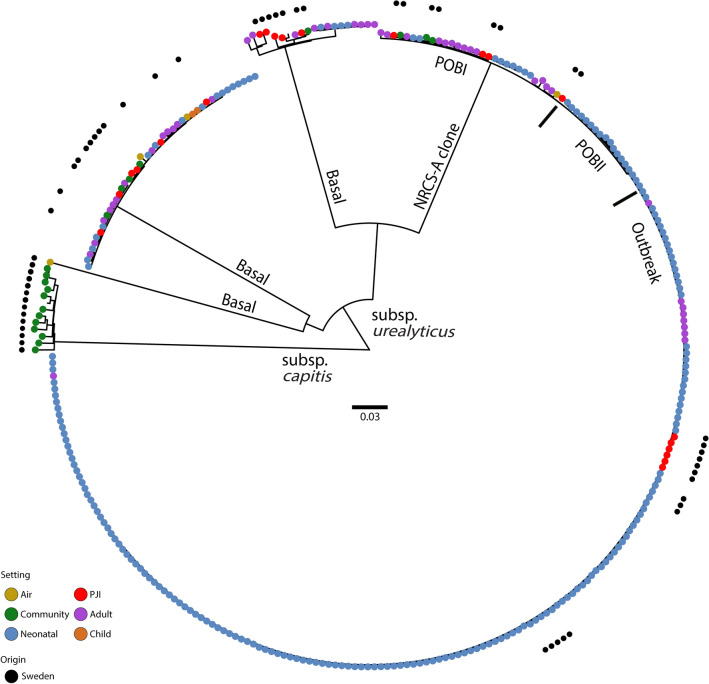
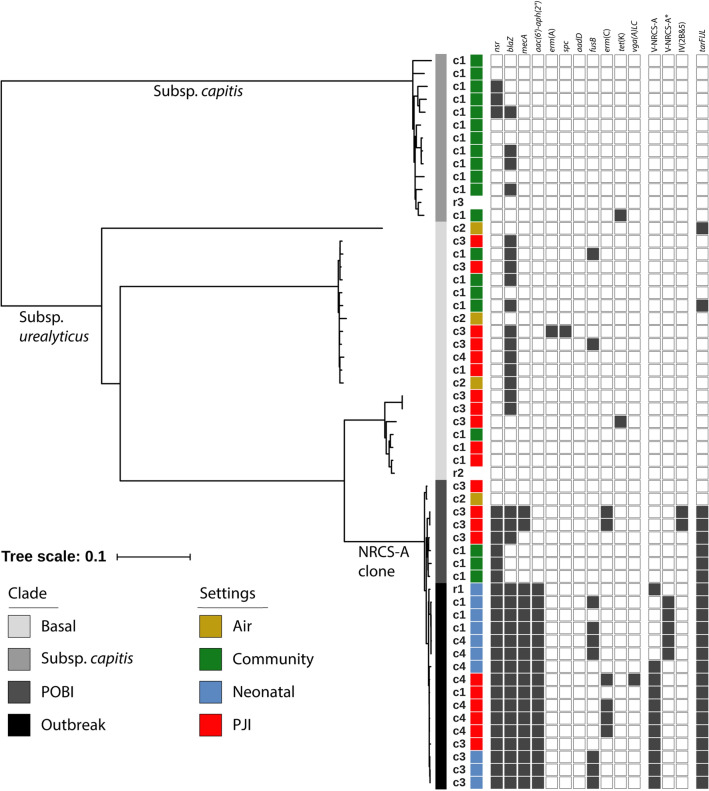
Staphylococcus capitis is a coagulase-negative staphylococcus that has been described primarily as causing bloodstream infections in neonatal intensive care units (NICUs), but has also recently been described in prosthetic joint infections (PJIs). The multidrug-resistant S. capitis subsp. urealyticus clone NRCS-A, comprising three sublineages, is prevalent in NICUs across the world, but its impact on other patient groups such as those suffering from PJIs or among adults planned for arthroplasty is unknown. Genome sequencing and subsequent analysis were performed on a Swedish collection of PJI isolates (n = 21), nasal commensals from patients planned to undergo arthroplasty (n = 20), NICU blood isolates (n = 9), operating theatre air isolates (n = 4), and reference strains (n = 2), in conjunction with an international strain collection (n = 248). The NRCS-A Outbreak sublineage containing the composite type V SCCmec-SCCcad/ars/cop element was present in PJIs across three Swedish hospitals. However, it was not found among nasal carrier strains, where the less virulent S. capitis subsp. capitis was most prevalent. The presence of the NRCS-A Outbreak clone in adult patients with PJIs demonstrates that dissemination occurs beyond NICUs. As this clone has several properties which facilitate invasive infections in patients with medical implants or immunosuppression, such as biofilm forming ability and multidrug resistance including heterogeneous glycopeptide-intermediate susceptibility, further research is needed to understand the reservoirs and distribution of this hospital-associated pathogen.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Kurtz SM, Lau E, Watson H, Schmier JK, Parvizi J. Economic burden of periprosthetic joint infection in the United States. J Arthroplasty. 2012;27(8 Suppl):61-5 e1. - PubMed
-
- Peel TN, Cole NC, Dylla BL, Patel R. Matrix-assisted laser desorption ionization time of flight mass spectrometry and diagnostic testing for prosthetic joint infection in the clinical microbiology laboratory. Diagn. Microbiol. Infect. Dis. 2015;81(3):163–168. doi: 10.1016/j.diagmicrobio.2014.11.015. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials
