

Germline Cancer Predisposition Variants in Pediatric Rhabdomyosarcoma: A Report From the Children's Oncology Group
- PMID: 33372952
- PMCID: PMC8246828
- DOI: 10.1093/jnci/djaa204
Germline Cancer Predisposition Variants in Pediatric Rhabdomyosarcoma: A Report From the Children's Oncology Group
Abstract
Background: Several cancer-susceptibility syndromes are reported to underlie pediatric rhabdomyosarcoma (RMS); however, to our knowledge there have been no systematic efforts to characterize the heterogeneous genetic etiologies of this often-fatal malignancy.
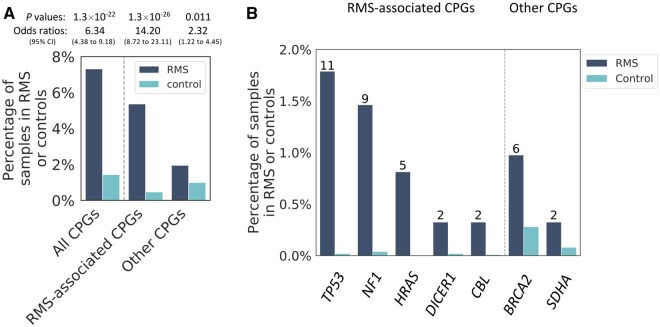
Methods: We performed exome-sequencing on germline DNA from 615 patients with newly diagnosed RMS consented through the Children's Oncology Group. We compared the prevalence of cancer predisposition variants in 63 autosomal-dominant cancer predisposition genes in these patients with population controls (n = 9963). All statistical tests were 2-sided.
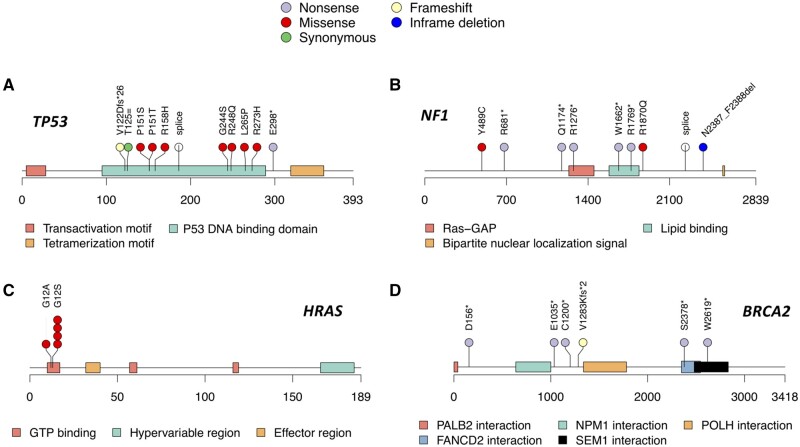
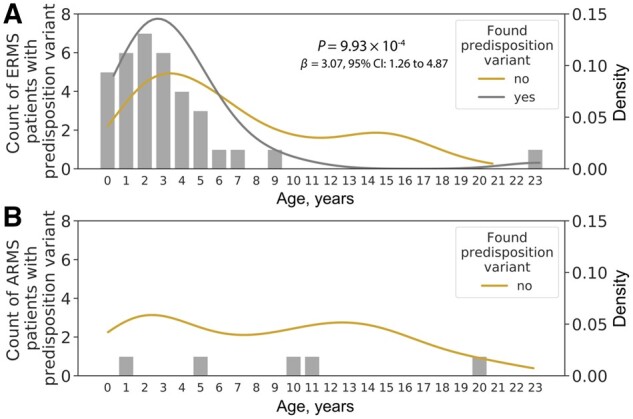
Results: We identified germline cancer predisposition variants in 45 RMS patients (7.3%; all FOXO1 fusion negative) across 15 autosomal dominant genes, which was statistically significantly enriched compared with controls (1.4%, P = 1.3 × 10-22). Specifically, 73.3% of the predisposition variants were found in predisposition syndrome genes previously associated with pediatric RMS risk, such as Li-Fraumeni syndrome (TP53) and neurofibromatosis type I (NF1). Notably, 5 patients had well-described oncogenic missense variants in HRAS (p.G12V and p.G12S) associated with Costello syndrome. Also, genetic etiology differed with histology, as germline variants were more frequent in embryonal vs alveolar RMS patients (10.0% vs 3.0%, P = .02). Although patients with a cancer predisposition variant tended to be younger at diagnosis (P = 9.9 × 10-4), 40.0% of germline variants were identified in those older than 3 years of age, which is in contrast to current genetic testing recommendations based on early age at diagnosis.
Conclusions: These findings demonstrate that genetic risk of RMS results from germline predisposition variants associated with a wide spectrum of cancer susceptibility syndromes. Germline genetic testing for children with RMS should be informed by RMS subtypes and not be limited to only young patients.
© The Author(s) 2020. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Ries LS, Gurney JG, Linet M, Tamra T, Young JL, Bunin GR.. Cancer Incidence and Survival Among Children and Adolescents: United States SEER Program 1975-1995, National Cancer Institute, SEER Program. Bethesda, MD: NIH Pub. No. 99-4649; 1999.
-
- Newton WA Jr., Gehan EA, Webber BL, et al.Classification of rhabdomyosarcomas and related sarcomas. Pathologic aspects and proposal for a new classification--an intergroup rhabdomyosarcoma study. Cancer. 1995;76(6):1073–1085. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
Miscellaneous
