

Performance of Digital Breast Tomosynthesis, Synthetic Mammography, and Digital Mammography in Breast Cancer Screening: A Systematic Review and Meta-Analysis
- PMID: 33372954
- PMCID: PMC8168096
- DOI: 10.1093/jnci/djaa205
Performance of Digital Breast Tomosynthesis, Synthetic Mammography, and Digital Mammography in Breast Cancer Screening: A Systematic Review and Meta-Analysis
Abstract
Background: Our objective was to perform a systematic review and meta-analysis comparing the breast cancer detection rate (CDR), invasive CDR, recall rate, and positive predictive value 1 (PPV1) of digital mammography (DM) alone, combined digital breast tomosynthesis (DBT) and DM, combined DBT and synthetic 2-dimensional mammography (S2D), and DBT alone.
Methods: MEDLINE and Embase were searched until April 2020 to identify comparative design studies reporting on patients undergoing routine breast cancer screening. Random effects model proportional meta-analyses estimated CDR, invasive CDR, recall rate, and PPV1. Meta-regression modeling was used to compare imaging modalities. All statistical tests were 2-sided.
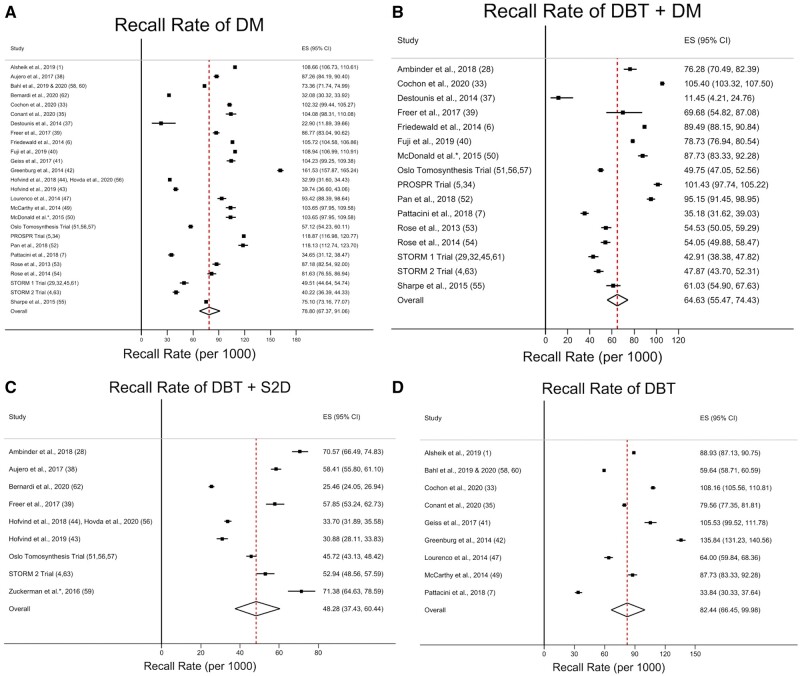
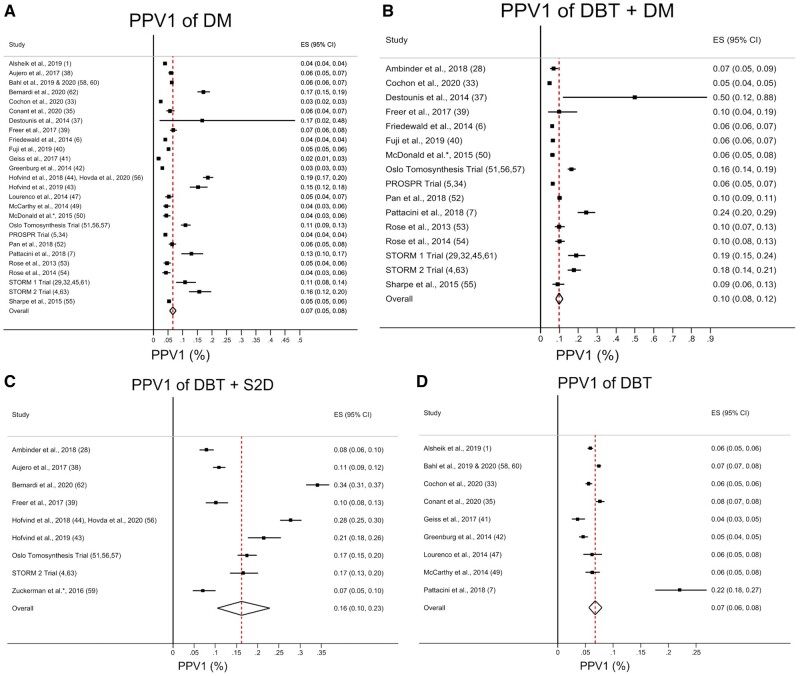
Results: Forty-two studies reporting on 2 606 296 patients (13 003 breast cancer cases) were included. CDR was highest in combined DBT and DM (6.36 per 1000 screened, 95% confidence interval [CI] = 5.62 to 7.14, P < .001), and combined DBT and S2D (7.40 per 1000 screened, 95% CI = 6.49 to 8.37, P < .001) compared with DM alone (4.68 per 1000 screened, 95% CI = 4.28 to 5.11). Invasive CDR was highest in combined DBT and DM (4.53 per 1000 screened, 95% CI = 3.97 to 5.12, P = .003) and combined DBT and S2D (5.68 per 1000 screened, 95% CI = 4.43 to 7.09, P < .001) compared with DM alone (3.42 per 1000 screened, 95% CI = 3.02 to 3.83). Recall rate was lowest in combined DBT and S2D (42.3 per 1000 screened, 95% CI = 37.4 to 60.4, P<.001). PPV1 was highest in combined DBT and DM (10.0%, 95% CI = 8.0% to 12.0%, P = .004), and combined DBT and S2D (16.0%, 95% CI = 10.0% to 23.0%, P < .001), whereas no difference was detected for DBT alone (7.0%, 95% CI = 6.0% to 8.0%, P = .75) compared with DM alone (7.0%, 95.0% CI = 5.0% to 8.0%).
Conclusions: Our findings provide evidence on key performance metrics for DM, DBT alone, combined DBT and DM, and combined DBT and S2D, which may inform optimal application of these modalities for breast cancer screening.
© The Author(s) 2020. Published by Oxford University Press. All rights reserved. For permissions, please email: journals.permissions@oup.com.
Figures



References
-
- Alsheik NH, Dabbous F, Pohlman SK, et al. Comparison of resource utilization and clinical outcomes following screening with digital breast tomosynthesis versus digital mammography: findings from a learning health system. Acad Radiol. 2019;26(5):597–605. - PubMed
-
- Boroumand G, Teberian I, Parker L, Rao VM, Levin DC. Screening mammography and digital breast tomosynthesis: utilization updates. Am J Roentgenol. 2018;210(5):1092–1096. - PubMed
-
- Sardanelli F, Fallenberg EM, Clauser P, et al. ; for the European Society of Breast Imaging (EUSOBI), with language review by Europa Donna-The European Breast Cancer Coalition. Mammography: an update of the EUSOBI recommendations on information for women. Insights Imaging. 2017;8(1):11–18. - PMC - PubMed
-
- Bernardi D, Macaskill P, Pellegrini M, et al. Breast cancer screening with tomosynthesis (3D mammography) with acquired or synthetic 2D mammography compared with 2D mammography alone (STORM-2): a population-based prospective study. Lancet Oncol. 2016;17(8):1105–1113. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
