

Spectrum of Disease Severity in Patients With X-Linked Retinitis Pigmentosa Due to RPGR Mutations
- PMID: 33372982
- PMCID: PMC7774109
- DOI: 10.1167/iovs.61.14.36
Spectrum of Disease Severity in Patients With X-Linked Retinitis Pigmentosa Due to RPGR Mutations
Abstract
Purpose: The purpose of this study was to perform a detailed longitudinal phenotyping of X-linked retinitis pigmentosa (RP) caused by mutations in the RPGR gene during a long follow-up period.
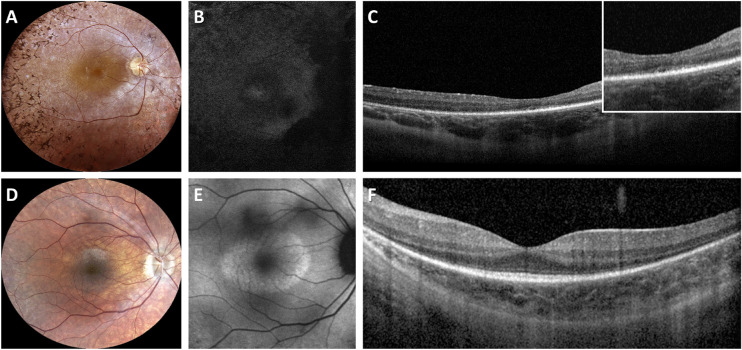
Methods: An Italian cohort of 48 male patients (from 31 unrelated families) with RPGR-associated RP was clinically assessed at a single center (mean follow-up = 6.5 years), including measurements of best-corrected visual acuity (BCVA), Goldmann visual field (GVF), optical coherence tomography (OCT), fundus autofluorescence (FAF), microperimetry, and full-field electroretinography (ERG).
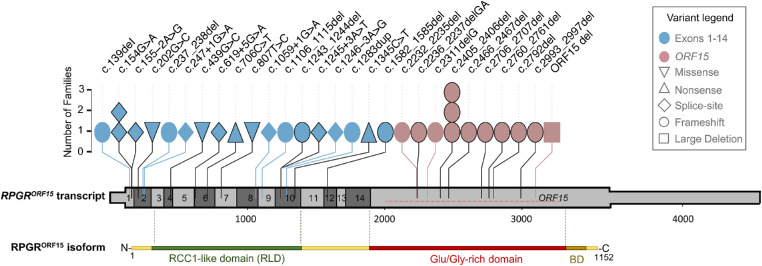
Results: Patients (29.6 ± 15.2 years) showed a mean BCVA of 0.6 ± 0.7 logMAR, mostly with myopic refraction (79.2%). Thirty patients (62.5%) presented a typical RP fundus, while the remaining sine pigmento RP. Over the follow-up, BCVA significantly declined at a mean rate of 0.025 logMAR/year. Typical RP and high myopia were associated with a significantly faster decline of BCVA. Blindness was driven primarily by GVF loss. ERG responses with a rod-cone pattern of dysfunction were detectable in patients (50%) that were significantly younger and more frequently presented sine pigmento RP. Thirteen patients (27.1%) had macular abnormalities without cystoid macular edema. Patients (50%) with a perimacular hyper-FAF ring were significantly younger, had a higher BCVA and a better-preserved ellipsoid zone band than those with markedly decreased FAF. Patients harboring pathogenic variants in exons 1 to 14 showed a milder phenotype compared to those with ORF15 mutations.
Conclusions: Our monocentric, longitudinal retrospective study revealed a spectrum disease progression in male patients with RPGR-associated RP. Slow disease progression correlated with sine pigmento RP, absence of high myopia, and mutations in RPGR exons 1 to 14.
Conflict of interest statement
Disclosure:
Figures

References
-
- Lyraki R, Megaw R, Hurd T.. Disease mechanisms of X-linked retinitis pigmentosa due to RP2 and RPGR mutations. Biochem Soc Trans. 2016; 44: 1235–1244. - PubMed
-
- Tee JJ, Smith AJ, Hardcastle AJ, Michaelides M.. RPGR-associated retinopathy: clinical features, molecular genetics, animal models and therapeutic options. Br J Ophthalmol. 2016; 100: 1022–1027. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
