

Prognostic significance of body temperature in the emergency department vs the ICU in Patients with severe sepsis or septic shock: A nationwide cohort study
- PMID: 33373376
- PMCID: PMC7771849
- DOI: 10.1371/journal.pone.0243990
Prognostic significance of body temperature in the emergency department vs the ICU in Patients with severe sepsis or septic shock: A nationwide cohort study
Abstract
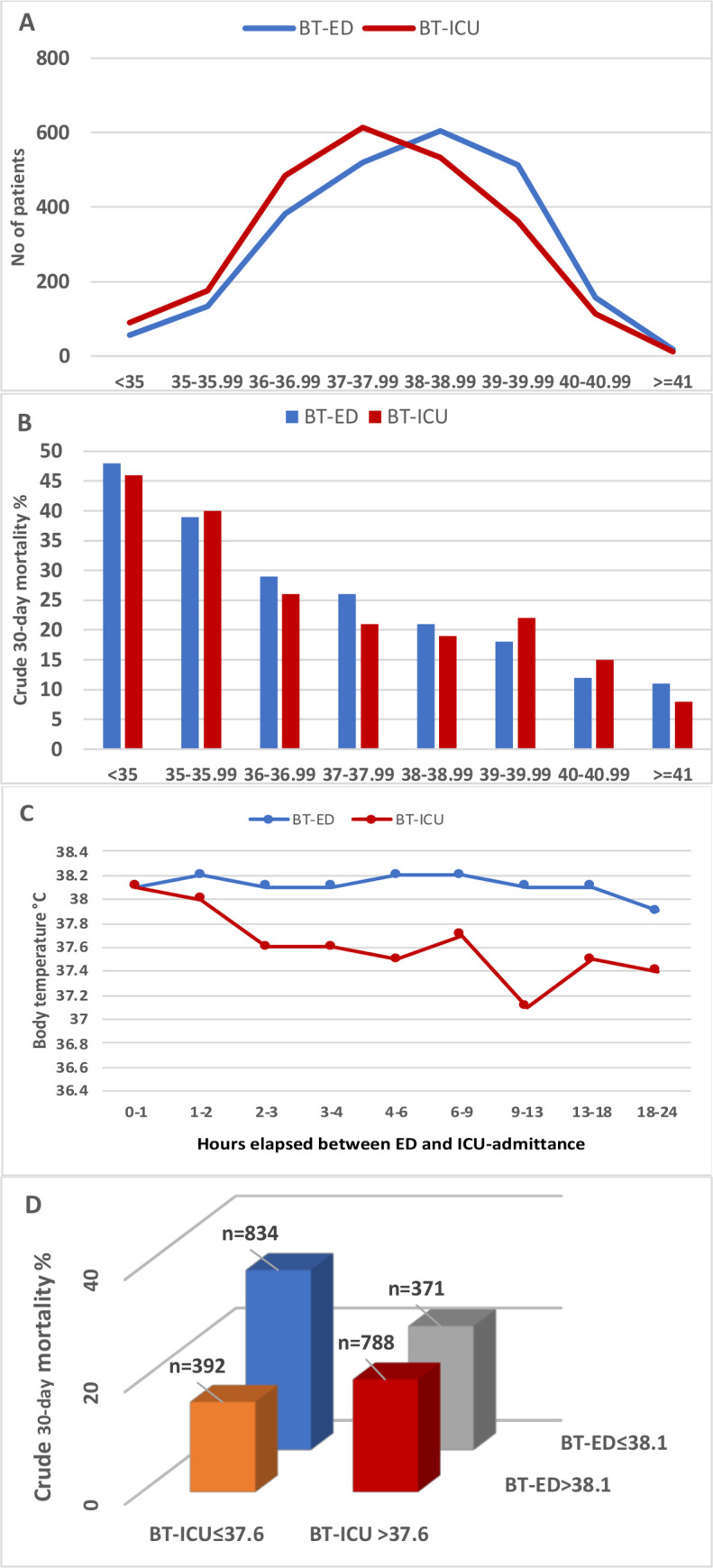
Background: Increased body temperature in the Emergency Department (BT-ED) and the ICU (BT-ICU) is associated with lower mortality in patients with sepsis. Here, we compared how well BT-ED and BT-ICU predict mortality; investigated mortality in various combinations of BT-ED and BT-ICU, and; compared degree of fever in the ED and ICU and associated quality of care.
Methods: 2385 adults who were admitted to an ICU within 24 hours of ED arrival with severe sepsis or septic shock were included.
Results: Thirty-day mortality was 23.6%. Median BT-ED and BT-ICU was 38.1 and 37.6°C. Crude mortality decreased more than 5% points per°C increase for both BT-ED and BT-ICU. Adjusted OR for mortality was 0.82/°C increase for BT-ED (0.76-0.88, p < 0.001), and 0.89 for BT-ICU (0.83-0.95, p<0.001). Patients who were at/below median temperature in both the ED and in the ICU had the highest mortality, 32%, and those with over median in the ED and at/below in the ICU had the lowest, 16%, (p<0.001). Women had 0.2°C lower median BT-ED (p = 0.03) and 0.3°C lower BT-ICU (p<0.0001) than men. Older patients had lower BT in the ICU, but not in the ED. Fever was associated with a higher rate of sepsis bundle achievement in the ED, but lower nurse workload in the ICU.
Conclusions: BT-ED was more useful to prognosticate mortality than BT-ICU. Despite better prognosis in patients with elevated BT, fever was associated with higher quality of care in the ED. Future studies should assess how BT-ED can be used to improve triage of infected patients, assigning higher priority to patients with low-grade/no fever and vice versa. Patients with at/below median BT in both ED and ICU have the highest mortality and should receive special attention. Different BT according to sex and age also needs further study.
Conflict of interest statement
The authors declare that no competing interests exist.
Figures


References
-
- Bryant RE, Hood AF, Hood CE, Koenig MG. Factors affecting mortality of gram-negative rod bacteremia. Arch Intern Med. 1971;127(1):120–8. - PubMed
-
- Weinstein MP, Towns ML, Quartey SM, Mirrett S, Reimer LG, Parmigiani G, et al. The clinical significance of positive blood cultures in the 1990s: a prospective comprehensive evaluation of the microbiology, epidemiology, and outcome of bacteremia and fungemia in adults. Clin Infect Dis. 1997;24(4):584–602. 10.1093/clind/24.4.584 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
