

Diagnostic Modality in Spine Disease: A Review
- PMID: 33373514
- PMCID: PMC7788365
- DOI: 10.31616/asj.2020.0593
Diagnostic Modality in Spine Disease: A Review
Abstract
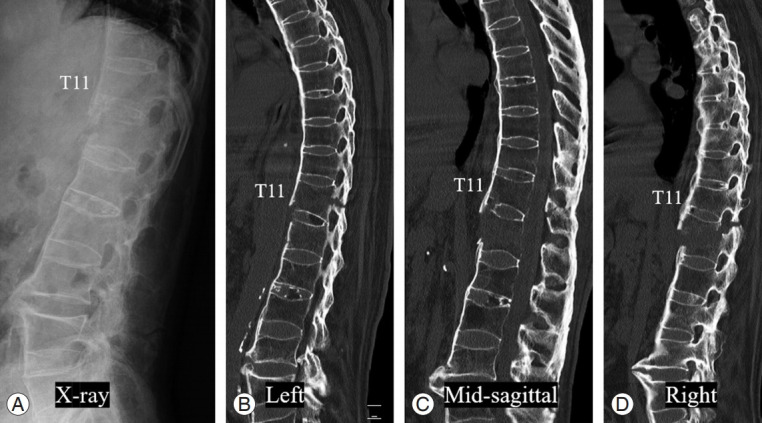
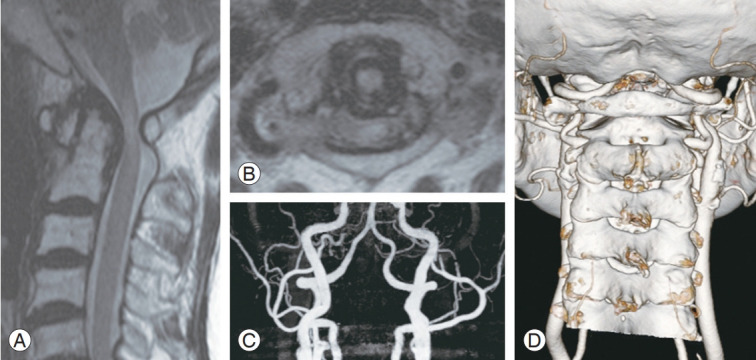
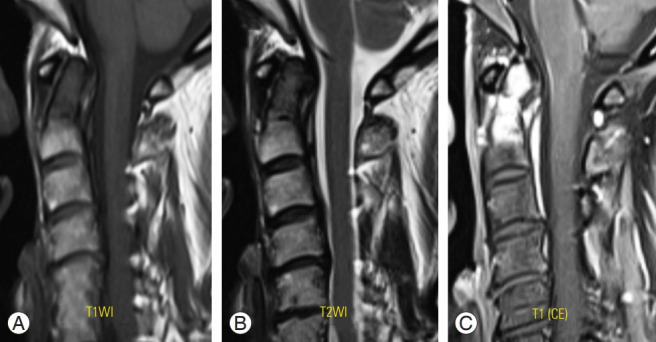
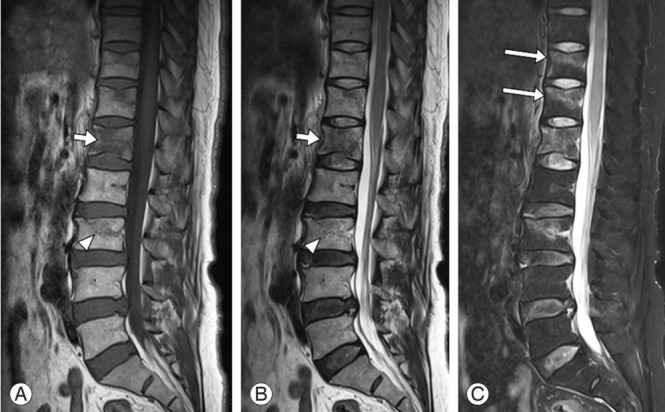
Spine diseases are common and exhibit several causes, including degeneration, trauma, congenital issues, and other specific factors. Most people experience a variety of symptoms of spine diseases during their lifetime that are occasionally managed with conservative or surgical treatments. Accurate diagnosis of the spine pathology is essential for the appropriate management of spine disease, and various imaging modalities can be used for the diagnosis, including radiography, computed tomography (CT), magnetic resonance imaging (MRI), and other studies such as EOS, bone scan, single photon emission CT/CT, and electrophysiologic test. Patient (or case)-specific selection of the diagnostic modality is crucial; thus, we should be aware of basic information and approaches of the diagnostic modalities. In this review, we discuss in detail, about diagnostic modalities (radiography, CT, MRI, electrophysiologic study, and others) that are widely used for spine disease.
Keywords: Computed tomography; Diagnostic imaging; Electrophysiologic study; Magnetic resonance imaging; Radiography; Spinal diseases.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Leone A, Guglielmi G, Cassar-Pullicino VN, Bonomo L. Lumbar intervertebral instability: a review. Radiology. 2007;245:62–77. - PubMed
-
- Jahnke RW, Hart BL. Cervical stenosis, spondylosis, and herniated disc disease. Radiol Clin North Am. 1991;29:777–91. - PubMed
-
- Simon JE, Lukin RR. Diskogenic disease of the cervical spine. Semin Roentgenol. 1988;23:118–24. - PubMed
LinkOut - more resources
Full Text Sources
