

A rare diagnostic challenge in a female patient with a rapid recurrent pleural effusion: Autopsy revealed cardiac angiosarcoma with bilateral pleural and pulmonary metastases. A case report
- PMID: 33373923
- PMCID: PMC7776125
- DOI: 10.1016/j.ijscr.2020.12.034
A rare diagnostic challenge in a female patient with a rapid recurrent pleural effusion: Autopsy revealed cardiac angiosarcoma with bilateral pleural and pulmonary metastases. A case report
Abstract
Introduction: We present a very rare case with diffuse cardiac angiosarcoma. Because all symptoms are often non-specific, this diagnosis is difficult to establish. To our knowledge this is the first clinical description of this rare disease.
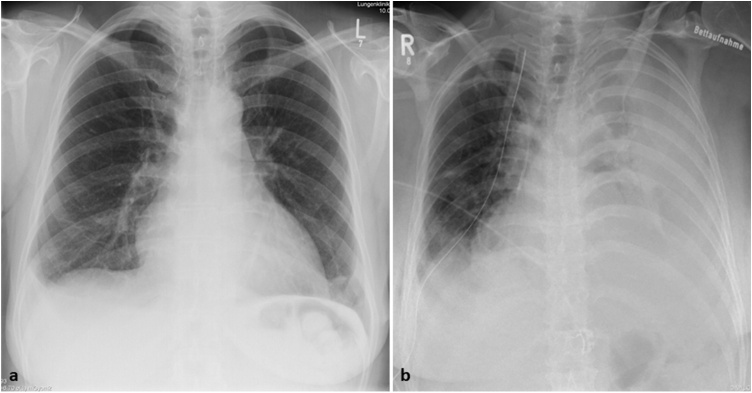
Presentation of case: A 47-year-old female presented with bilateral pulmonary infiltrates and non-specific symptoms as fever, chest pain and dyspnoea on exertion. She was treated with antibiotics for suspected lung infection but deteriorated developing rapid recurrent pleural effusion. Her transthoracic- and transoesophageal-echocardiography as well as the thoracentesis and endobronchial ultrasound findings were normal. A minimally invasive pulmonary wedge resection, partial pleurectomy and pericardial fenestration was performed. The pathologic interpretation of these specimen was very difficult and a correct diagnosis could be made only by the second reference pathologist. While awaiting reference histology report she was administered high-flow oxygen therapy for hypoxia, antibiotics, catecholamines and corticosteroids. The patient deteriorated very rapidly and died in the ICU.
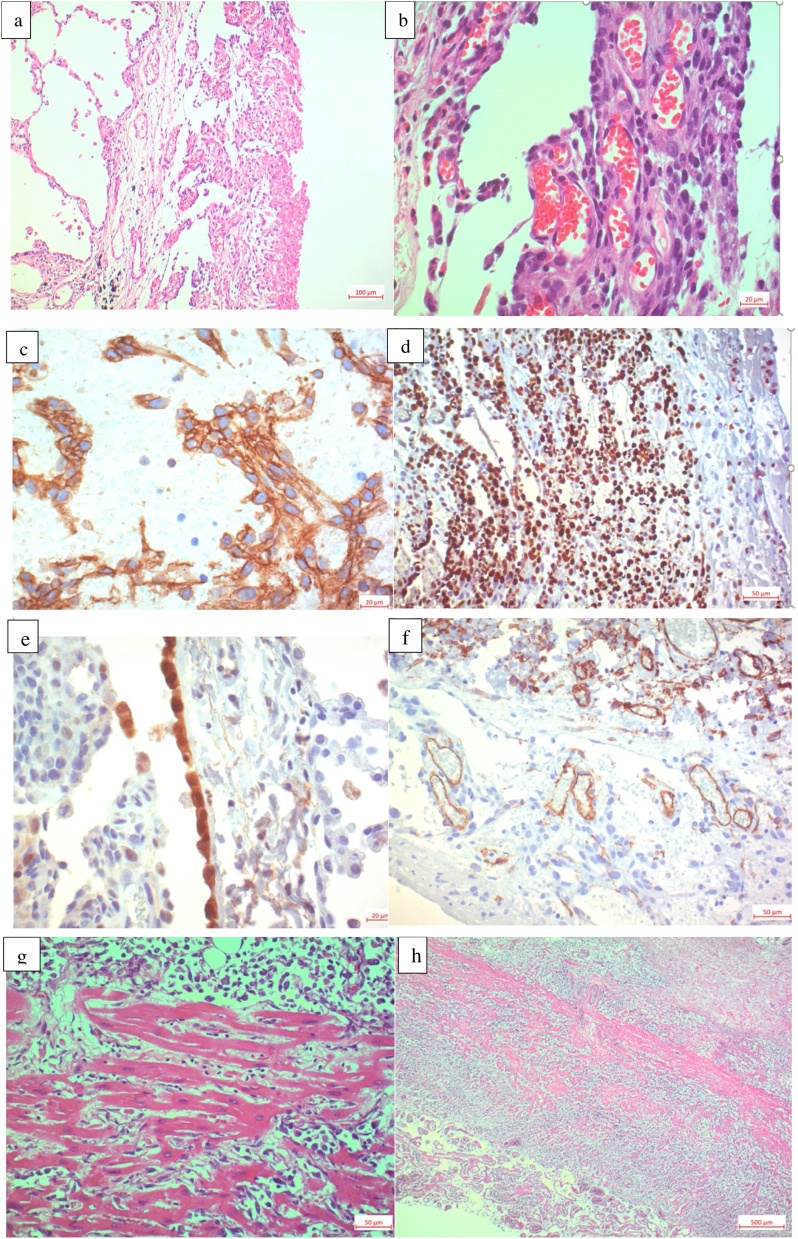
Discussion: As in earlier studies, misdiagnosis delayed the actual diagnosis, especially because there was no clinical suspicion for angiosarcoma. Pathologic evaluation may be difficult because different growth patterns may be present in the same tumour and pleural or lung specimen may show only very tiny tumour formations within a fibrosing tissue changes.
Conclusion: This case report highlights the difficulties to establish a diagnosis of diffuse angiosarcoma in time. An early diagnosis, to initiate oncologic treatment, require a high level of clinical suspicion and a histological proof from pericardial or myocardial biopsy.
Keywords: Autopsy; Cardiac angiosarcoma; Haemoptysis; Pulmonary infiltrates; Transoesophageal echocardiography.
Copyright © 2020 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures

References
-
- Burke A., Tavora F. The 2015 WHO Classification of tumors of the heart and pericardium. J. Thorac. Oncol. 2016 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
