

Microscopic Peritoneal Residual Disease after Complete Macroscopic Cytoreductive Surgery for Advanced High Grade Serous Ovarian Cancer
- PMID: 33375564
- PMCID: PMC7795826
- DOI: 10.3390/jcm10010041
Microscopic Peritoneal Residual Disease after Complete Macroscopic Cytoreductive Surgery for Advanced High Grade Serous Ovarian Cancer
Abstract
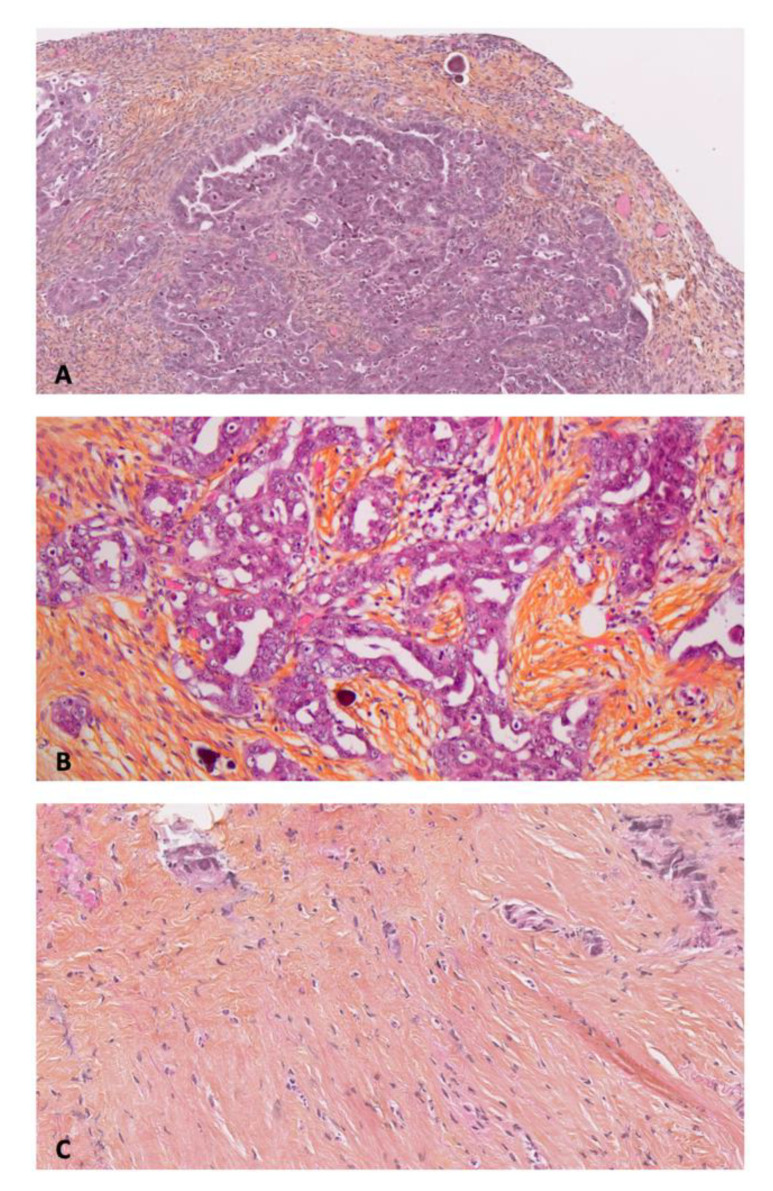
Background: Epithelial ovarian cancers (EOC) are usually diagnosed at an advanced stage and managed by complete macroscopic cytoreductive surgery (CRS) and systemic chemotherapy. Peritoneal recurrence occurs in 60% of patients and may be due to microscopic peritoneal metastases (mPM) which are neither eradicated by surgery nor controlled by systemic chemotherapy. The aim of this study was to assess and quantify the prevalence of residual mPM after complete macroscopic CRS in patients with advanced high-grade serous ovarian cancer (HGSOC).
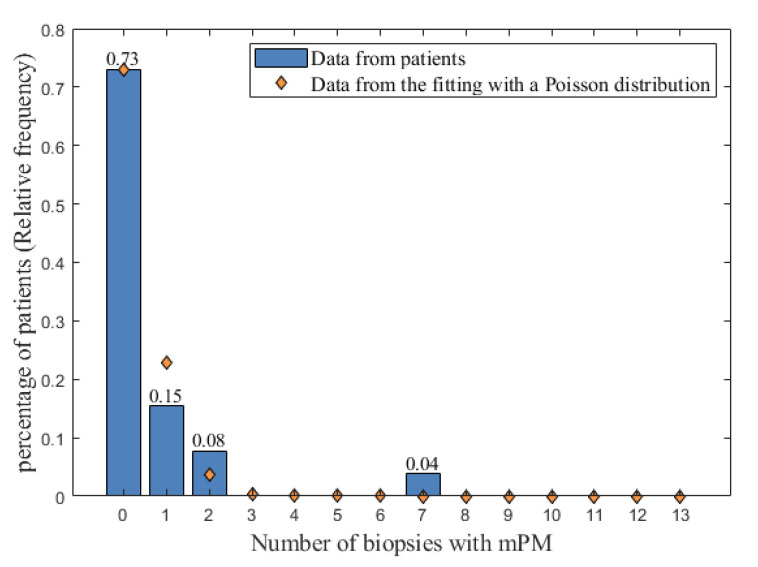
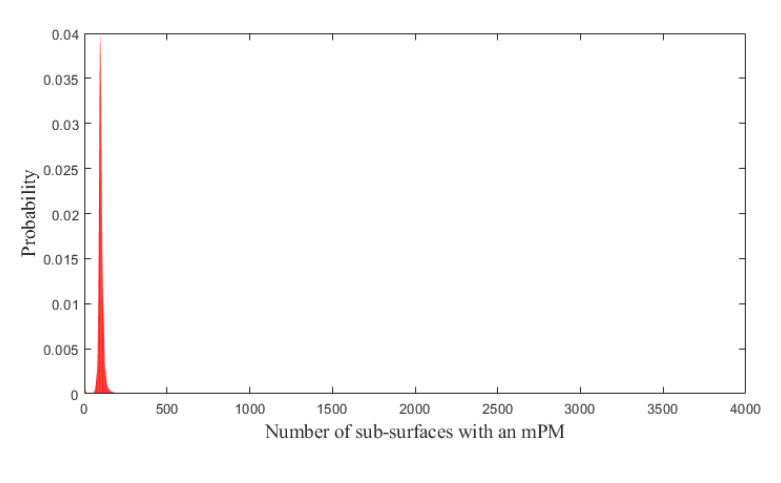
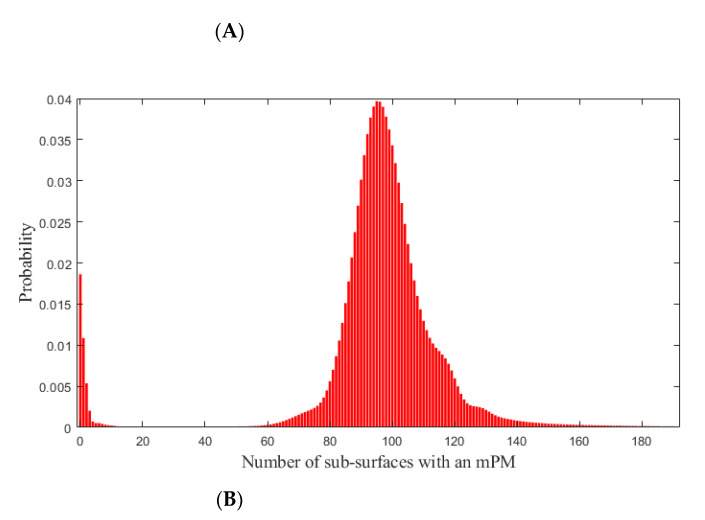
Methods: A prospective study conducted between 1 June 2018 and 10 July 2019 in a single referent center accredited by the European Society of Gynecological Oncology for advanced EOC management. Consecutive patients presenting with advanced HGSOC and eligible for complete macroscopic CRS were included. Up to 13 peritoneal biopsies were taken from macroscopically healthy peritoneum at the end of CRS and examined for the presence of mPM. A mathematical model was designed to determine the probability of presenting at least one mPM after CRS.
Results: 26 patients were included and 26.9% presented mPM. There were no differences in characteristics between patients with or without identified mPM. After mathematical analysis, the probability that mPM remained after complete macroscopic CRS in patients with EOC was 98.14%.
Conclusion: Microscopic PM is systematically present after complete macroscopic CRS for EOC and could be a relevant therapeutic target. Adjuvant locoregional strategies to conventional surgery may improve survival by achieving microscopic CRS.
Keywords: cytoreductive surgery; epithelial ovarian cancer; gynecologic oncology; peritoneal carcinomatosis.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
