

HER2 Status in High-Risk Endometrial Cancers (PORTEC-3): Relationship with Histotype, Molecular Classification, and Clinical Outcomes
- PMID: 33375706
- PMCID: PMC7795222
- DOI: 10.3390/cancers13010044
HER2 Status in High-Risk Endometrial Cancers (PORTEC-3): Relationship with Histotype, Molecular Classification, and Clinical Outcomes
Abstract
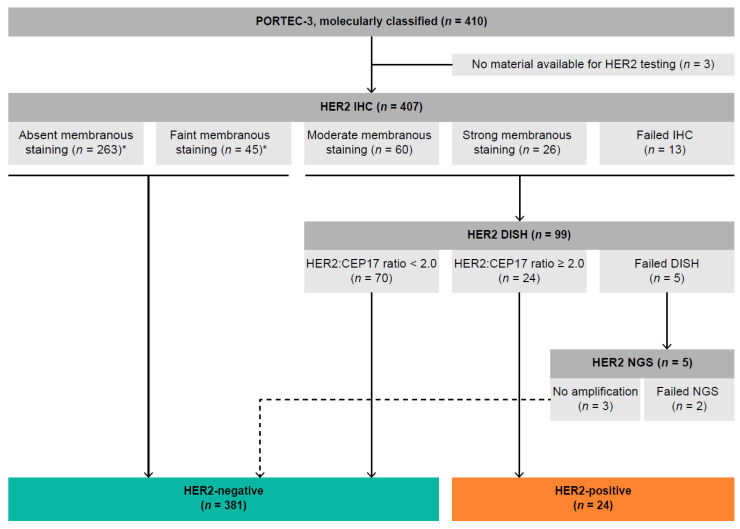
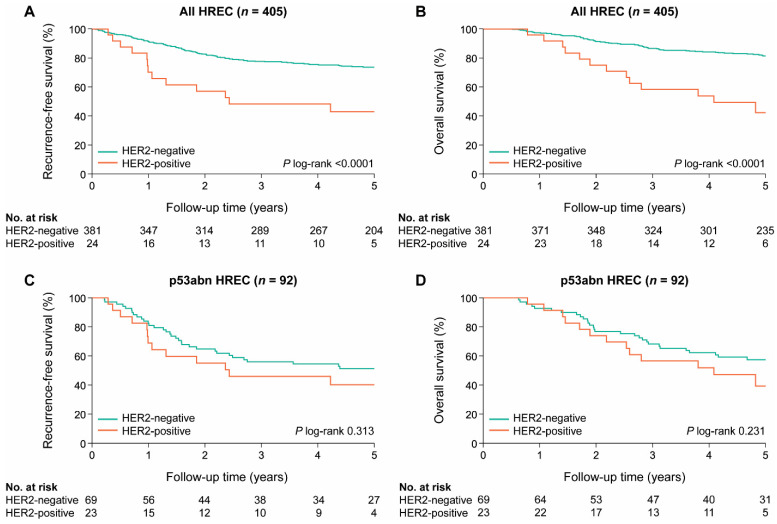
HER2 status has not been investigated in the context of the molecular endometrial cancer (EC) classification. Here, we aimed to determine the clinicopathological features and prognostic significance of the HER2 status in the molecularly classified PORTEC-3 trial population of patients with high-risk EC (HREC). HER2 testing was performed on tumor tissues of 407 molecularly classified HREC. HER2 status was determined by HER2 immunohistochemistry (IHC; all cases) and subsequent HER2 dual in situ hybridization for cases with any (in) complete moderate to strong membranous HER2 IHC expression. The Χ2 test and Spearman's Rho correlation coefficient were used to compare clinicopathological and molecular features. The Kaplan-Meier method, log-rank test, and Cox proportional hazards models were used for survival analysis. We identified 24 (5.9%) HER2-positive EC of various histological subtypes including serous (n = 9, 37.5%), endometrioid (n = 6, 25.0%), and clear cell (n = 5, 20.8%). HER2 positivity was highly associated with the p53-abnormal subgroup (p53abn, 23/24 cases; p < 0.0001). The correlation between p53abn and the HER2 status (ρ = 0.438; p < 0.0001) was significantly stronger (p < 0.0001) than between serous histology and the HER2 status (ρ = 0.154; p = 0.002). HER2 status did not have independent prognostic value for survival after correction for the molecular classification. Our study strongly suggests that molecular subclass-directed HER2 testing is superior to histotype-directed testing. This insight will be relevant for future trials targeting HER2.
Keywords: ERBB2; HER2; endometrial cancer; high-risk; p53.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Colombo N., Creutzberg C.L., Querleu D., Barahona M., Sessa C., Committee E.G. Appendix 5: Endometrial cancer: eUpdate published online 8 June 2017 (www.esmo.org/Guidelines/Gynaecological-Cancers) Ann. Oncol. 2017;28:iv153–iv156. doi: 10.1093/annonc/mdx243. - DOI - PubMed
-
- De Boer S., Powell M.E., Mileshkin L., Katsaros D., Bessette P., Haie-Meder C., Ottevanger P.B., Ledermann J.A., Khaw P., Colombo A., et al. Adjuvant chemoradiotherapy versus radiotherapy alone for women with high-risk endometrial cancer (PORTEC-3): Final results of an international, open-label, multicentre, randomised, phase 3 trial. Lancet Oncol. 2018;19:295–309. doi: 10.1016/S1470-2045(18)30079-2. - DOI - PMC - PubMed
-
- Bendifallah S., Canlorbe G., Collinet P., Arsene E., Huguet F., Coutant C., Hudry D., Graesslin O., Raimond E., Touboul C., et al. Just how accurate are the major risk stratification systems for early-stage endometrial cancer? Br. J. Cancer. 2015;112:793–801. doi: 10.1038/bjc.2015.35. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
