

Upfront middle meningeal artery embolization for treatment of chronic subdural hematomas in patients with or without midline shift
- PMID: 33375866
- PMCID: PMC8580532
- DOI: 10.1177/1591019920982816
Upfront middle meningeal artery embolization for treatment of chronic subdural hematomas in patients with or without midline shift
Abstract
Objectives: There is limited data on upfront middle meningeal artery (MMA) embolization in the context of significant midline shift (MLS) (greater than 5mm) for the treatment of chronic subdural hematomas (cSDH). This study reports the temporal changes following MMA embolization as an upfront treatment of cSDH in patients with or without MLS and either mild, no symptoms or mild and stable neurological deficits.
Methods: A retrospective series of patients with a cSDH from a single institution in the United States between 2018-2020 was conducted. Eligible patients were treated with upfront MMA embolization.
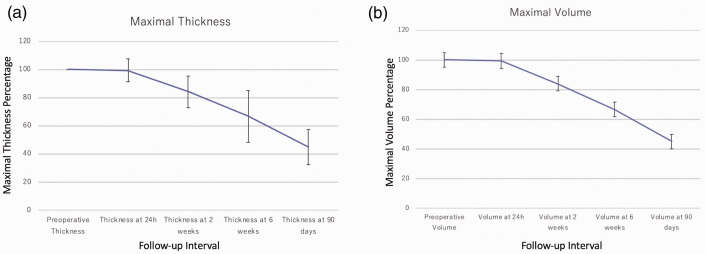
Results: 27 upfront MMA embolization procedures in 23 patients were included. Twelve patients had MLS of 5 millimeters or more (52%). The median maximal thickness at diagnosis was 18 mm [11-22]. The mean distance of MLS was 5 mm ±4. There were no procedural complications. The overall rescue surgery rate was 15%. A single rescue surgery secondary to an increase in hematoma thickness was required (4%). The temporal changes for both hematoma and MLS showed gradual improvement between 2 weeks and 4 weeks post-procedure. The average time-to-resolution of MLS was 46 days in patients with less than 5 mm MLS and 51 days in those with 5 mm or more.
Conclusion: Upfront MMA embolization for cSDH with a thickness up to 25 mm provides adequate symptom relief, stabilization and/or progressive resorption of the cSDH during follow-up in carefully selected asymptomatic or mildly symptomatic patients even in the presence of a MLS greater than 5 mm.
Keywords: Embolization; cerebrovascular; middle meningeal artery embolization; midline shift; subdural hematoma.
Conflict of interest statement
Figures


Similar articles
-
Subdural evacuation port system and middle meningeal artery embolization for chronic subdural hematoma: a multicenter experience.J Neurosurg. 2022 Nov 11;139(1):131-138. doi: 10.3171/2022.10.JNS221476. Print 2023 Jul 1. J Neurosurg. 2022. PMID: 36681990
-
Middle meningeal artery embolization as an adjuvant treatment to surgery for symptomatic chronic subdural hematoma: a pilot study assessing hematoma volume resorption.J Neurointerv Surg. 2020 Jul;12(7):695-699. doi: 10.1136/neurintsurg-2019-015421. Epub 2019 Dec 20. J Neurointerv Surg. 2020. PMID: 31862830 Clinical Trial.
-
Enhanced Hematoma Membrane on DynaCT Images During Middle Meningeal Artery Embolization for Persistently Recurrent Chronic Subdural Hematoma.World Neurosurg. 2019 Jun;126:e473-e479. doi: 10.1016/j.wneu.2019.02.074. Epub 2019 Feb 28. World Neurosurg. 2019. PMID: 30825631
-
Radiological Evaluation Criteria for Chronic Subdural Hematomas : Review of the Literature.Clin Neuroradiol. 2022 Dec;32(4):923-929. doi: 10.1007/s00062-022-01138-1. Epub 2022 Feb 14. Clin Neuroradiol. 2022. PMID: 35157088 Free PMC article. Review.
-
Middle Meningeal Artery Embolization for Primary Treatment of a Chronic Subdural Hematoma in a Pediatric Patient: A Systematic Review of the Literature and Case Report.Oper Neurosurg. 2023 Jan 1;24(1):3-10. doi: 10.1227/ons.0000000000000446. Epub 2022 Nov 3. Oper Neurosurg. 2023. PMID: 36519875
Cited by
-
Middle meningeal artery embolization with standalone or adjunctive coiling for treatment of chronic subdural hematoma: Systematic review and meta-analysis.Interv Neuroradiol. 2024 Dec 12:15910199241304852. doi: 10.1177/15910199241304852. Online ahead of print. Interv Neuroradiol. 2024. PMID: 39665194 Free PMC article. Review.
-
Safety and immediate outcomes of the new generation Swift PAC coil in cerebrovascular pathology: A case series.Interv Neuroradiol. 2025 May 21:15910199251343735. doi: 10.1177/15910199251343735. Online ahead of print. Interv Neuroradiol. 2025. PMID: 40398463 Free PMC article.
-
The Mini-Craniotomy for cSDH Revisited: New Perspectives.Front Neurol. 2021 May 6;12:660885. doi: 10.3389/fneur.2021.660885. eCollection 2021. Front Neurol. 2021. PMID: 34025564 Free PMC article.
-
Middle meningeal artery embolization for chronic subdural hematomas. A systematic review of the literature focused on indications, technical aspects, and future possible perspectives.Surg Neurol Int. 2022 Mar 18;13:94. doi: 10.25259/SNI_911_2021. eCollection 2022. Surg Neurol Int. 2022. PMID: 35399896 Free PMC article. Review.
-
Helical coils augment embolization of the middle meningeal artery for treatment of chronic subdural hematoma: A technical note.J Cerebrovasc Endovasc Neurosurg. 2023 Jun;25(2):214-223. doi: 10.7461/jcen.2023.E2022.08.001. Epub 2023 Jan 12. J Cerebrovasc Endovasc Neurosurg. 2023. PMID: 36632030 Free PMC article.
References
-
- Ducruet AF, Grobelny BT, Zacharia BE, et al.. The surgical management of chronic subdural hematoma. Neurosurg Rev 2012; 35: 155–169; discussion 169. - PubMed
-
- Miranda LB, Braxton E, Hobbs J, et al.. Chronic subdural hematoma in the elderly: not a benign disease. J Neurosurg 2011; 114: 72–76. - PubMed
-
- Almenawer SA, Farrokhyar F, Hong C, et al.. Chronic subdural hematoma management: a systematic review and meta-analysis of 34,829 patients. Ann Surg 2014; 259: 449–457. - PubMed
-
- Ivamoto HS Lemos HP JrandAtallah AN.. Surgical treatments for chronic subdural hematomas: a comprehensive systematic review. World Neurosurg 2016; 86: 399–418. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
