

Effect of medicines management versus standard care on readmissions in multimorbid patients: a randomised controlled trial
- PMID: 33376173
- PMCID: PMC7778779
- DOI: 10.1136/bmjopen-2020-041558
Effect of medicines management versus standard care on readmissions in multimorbid patients: a randomised controlled trial
Abstract
Objective: To investigate the effect of pharmacist-led medicines management in multimorbid, hospitalised patients on long-term hospital readmissions and survival.
Design: Parallel-group, randomised controlled trial.
Setting: Recruitment from an internal medicine hospital ward in Oslo, Norway. Patients were enrolled consecutively from August 2014 to the predetermined target number of 400 patients. The last participant was enrolled March 2016. Follow-up until 31 December 2017, that is, 21-40 months.
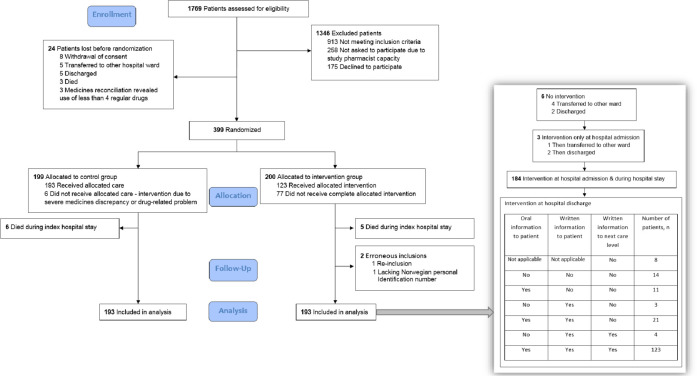
Participants: Acutely admitted multimorbid patients ≥18 years, using minimum four regular drugs from minimum two therapeutic classes. 399 patients were randomly assigned, 1:1, to the intervention or control group. After excluding 11 patients dying in-hospital and 2 erroneously included, the primary analysis comprised 386 patients (193 in each group) with median age 79 years (range 23-96) and number of diseases 7 (range 2-17).
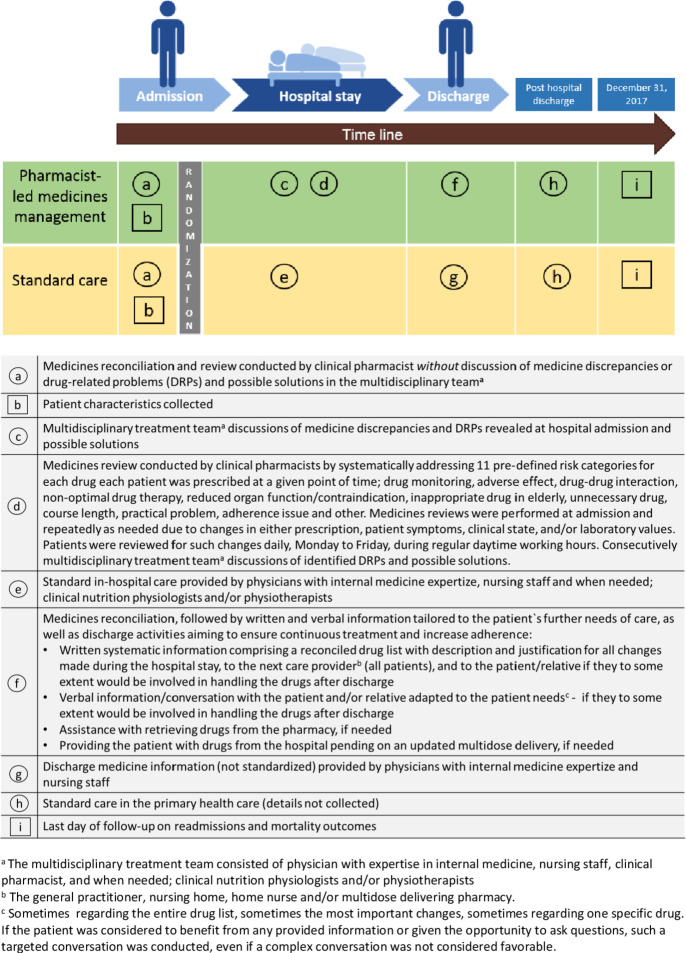
Intervention: Intervention patients received pharmacist-led medicines management comprising medicines reconciliation at admission, repeated medicines reviews throughout the stay and medicines reconciliation and tailored information at discharge, according to the integrated medicines management model. Control patients received standard care.
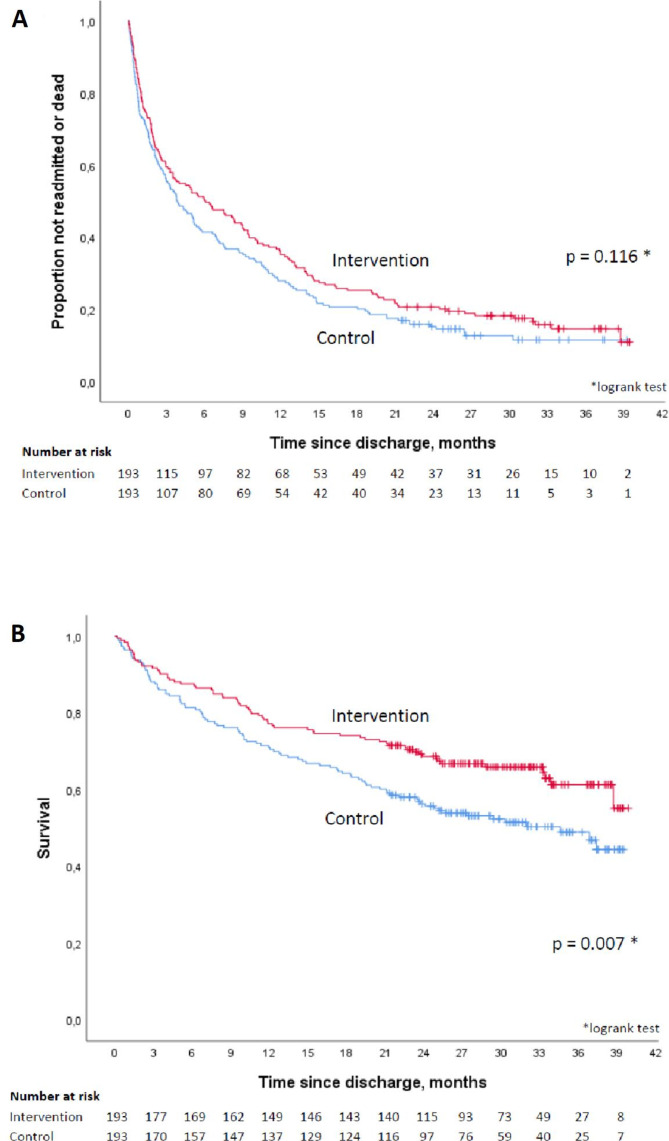
Primary and secondary outcome measures: The primary endpoint was difference in time to readmission or death within 12 months. Overall survival was a priori the clinically most important secondary endpoint.
Results: Pharmacist-led medicines management had no significant effect on the primary endpoint time to readmission or death within 12 months (median 116 vs 184 days, HR 0.82, 95% CI 0.64 to 1.04, p=0.106). A statistically significantly increased overall survival was observed during 21-40 months follow-up (HR 0.66, 95% CI 0.48 to 0.90, p=0.008).
Conclusions: Pharmacist-led medicines management had no statistically significant effect on time until readmission or death. A statistically significant increased overall survival was seen. Further studies should be conducted to investigate the effect of such an intervention on a larger scale.
Trial registration number: NCT02336113.
Keywords: clinical pharmacology; internal medicine; public health; quality in health care; therapeutics.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: ML received Ph.D. funding from the South-Eastern Norway Regional Health Authority (grant number 12/00718).
Figures
References
-
- Mercer S, Salisbury C, Fortin M. Abc of multimorbidity. first ED. John Wiley & Sons, 2014.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical