

Interpreting the Lancet surgical indicators in Somaliland: a cross-sectional study
- PMID: 33376180
- PMCID: PMC7778782
- DOI: 10.1136/bmjopen-2020-042968
Interpreting the Lancet surgical indicators in Somaliland: a cross-sectional study
Abstract
Background: The unmet burden of surgical care is high in low-income and middle-income countries. The Lancet Commission on Global Surgery (LCoGS) proposed six indicators to guide the development of national plans for improving and monitoring access to essential surgical care. This study aimed to characterise the Somaliland surgical health system according to the LCoGS indicators and provide recommendations for next-step interventions.
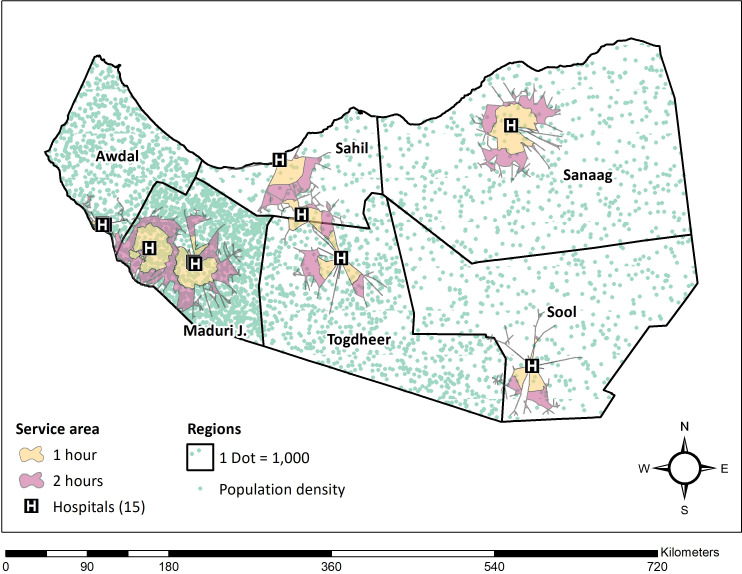
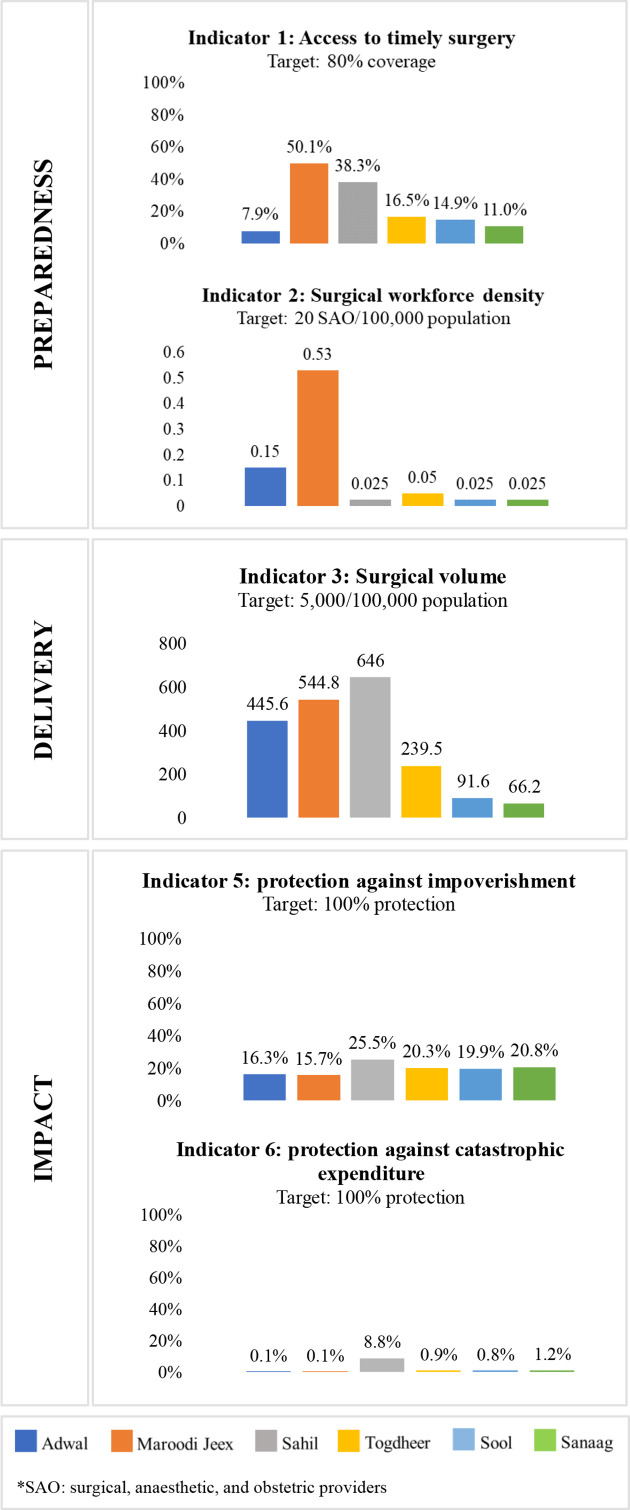
Methods: In this cross-sectional nationwide study, the WHO's Surgical Assessment Tool-Hospital Walkthrough and geographical mapping were used for data collection at 15 surgically capable hospitals. LCoGS indicators for preparedness was defined as access to timely surgery and specialist surgical workforce density (surgeons, anaesthesiologists and obstetricians/SAO), delivery was defined as surgical volume, and impact was defined as protection against impoverishment and catastrophic expenditure. Indicators were compared with the LCoGS goals and were stratified by region.
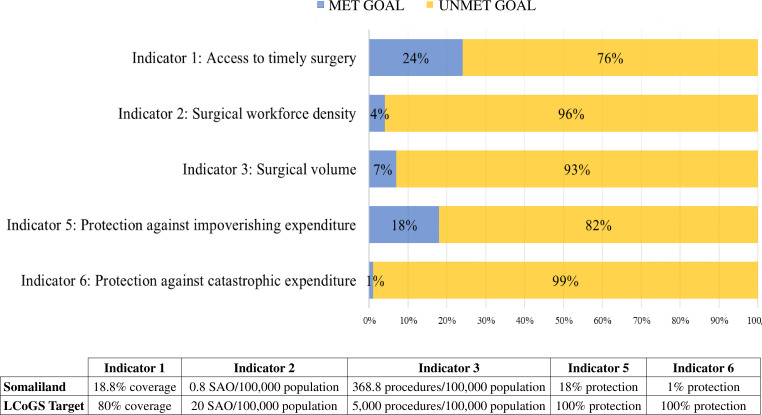
Results: The healthcare system in Somaliland does not meet any of the six LCoGS targets for preparedness, delivery or impact. We estimate that only 19% of the population has timely access to essential surgery, less than the LCoGS goal of 80% coverage. The number of specialist SAO providers is 0.8 per 100 000, compared with an LCoGS goal of 20 SAO per 100 000. Surgical volume is 368 procedures per 100 000 people, while the LCoGS goal is 5000 procedures per 100 000. Protection against impoverishing expenditures was only 18% and against catastrophic expenditures 1%, both far below the LCoGS goal of 100% protection.
Conclusion: We found several gaps in the surgical system in Somaliland using the LCoGS indicators and target goals. These metrics provide a broad view of current status and gaps in surgical care, and can be used as benchmarks of progress towards universal health coverage for the provision of safe, affordable, and timely surgical, obstetric and anaesthesia care in Somaliland.
Keywords: health policy; international health services; public health; surgery.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: For the original study on which this article is based, TC and ERS received grants from Duke University’s Duke Global Health Institute and grants from Baylor University.
Figures
Similar articles
-
An Evaluation of Preparedness, Delivery and Impact of Surgical and Anesthesia Care in Madagascar: A Framework for a National Surgical Plan.World J Surg. 2017 May;41(5):1218-1224. doi: 10.1007/s00268-016-3847-9. World J Surg. 2017. PMID: 27905017
-
Use of the six core surgical indicators from the Lancet Commission on Global Surgery in Colombia: a situational analysis.Lancet Glob Health. 2020 May;8(5):e699-e710. doi: 10.1016/S2214-109X(20)30090-5. Lancet Glob Health. 2020. PMID: 32353317
-
A Narrative Review of Kenya's Surgical Capacity Using the Lancet Commission on Global Surgery's Indicator Framework.Glob Health Sci Pract. 2022 Feb 28;10(1):e2100500. doi: 10.9745/GHSP-D-21-00500. Print 2022 Feb 28. Glob Health Sci Pract. 2022. PMID: 35294388 Free PMC article. Review.
-
Assessing Ethiopia's surgical capacity in light of global surgery 2030 initiatives: Is there progress in the past decade?Surg Open Sci. 2024 Mar 28;19:70-79. doi: 10.1016/j.sopen.2024.03.015. eCollection 2024 Jun. Surg Open Sci. 2024. PMID: 38595832 Free PMC article. Review.
-
Universal access to safe, affordable, timely surgical and anaesthetic care in Papua New Guinea: the six global health indicators.ANZ J Surg. 2020 Oct;90(10):1903-1909. doi: 10.1111/ans.16148. Epub 2020 Jul 20. ANZ J Surg. 2020. PMID: 33710739
Cited by
-
Assessment of anesthesia capacity for children in Somaliland.PLOS Glob Public Health. 2024 Aug 28;4(8):e0003650. doi: 10.1371/journal.pgph.0003650. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 39196977 Free PMC article.
-
Association between ambulance prehospital time and maternal and perinatal outcomes in Sierra Leone: a countrywide study.BMJ Glob Health. 2021 Nov;6(11):e007315. doi: 10.1136/bmjgh-2021-007315. BMJ Glob Health. 2021. PMID: 34844999 Free PMC article.
-
The state of global surgery assessment and data collection tools: A scoping review.World J Surg. 2024 Dec;48(12):2972-2989. doi: 10.1002/wjs.12380. Epub 2024 Oct 28. World J Surg. 2024. PMID: 39467820 Free PMC article.
-
Delays in care for hydrocephalus and spina bifida at a tertiary hospital in Somaliland.World J Pediatr Surg. 2023 Jan 20;6(1):e000472. doi: 10.1136/wjps-2022-000472. eCollection 2023. World J Pediatr Surg. 2023. PMID: 38328393 Free PMC article.
-
Letter to Editor: Are LMICs Achieving the Lancet Commission Global Benchmark for Surgical Volumes? A Systematic Review.World J Surg. 2023 Dec;47(12):3437-3438. doi: 10.1007/s00268-023-07136-9. Epub 2023 Aug 1. World J Surg. 2023. PMID: 37528271 No abstract available.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical