

Clinical features of BK-polyomavirus and cytomegalovirus co-infection after kidney transplantation
- PMID: 33376243
- PMCID: PMC7772341
- DOI: 10.1038/s41598-020-79799-6
Clinical features of BK-polyomavirus and cytomegalovirus co-infection after kidney transplantation
Abstract
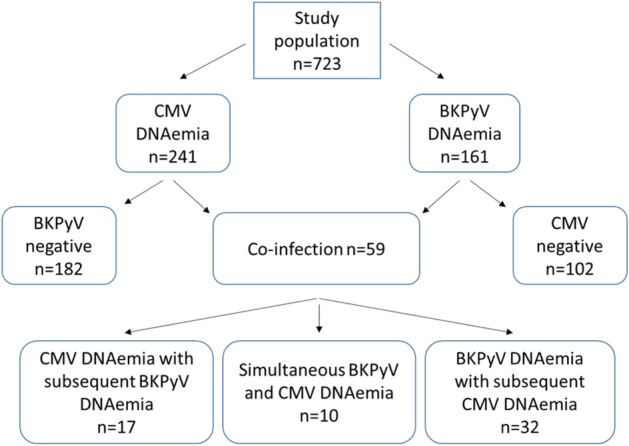
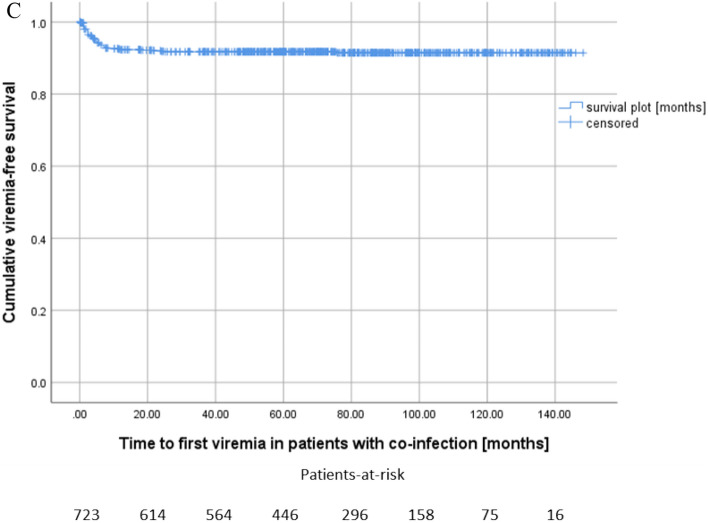
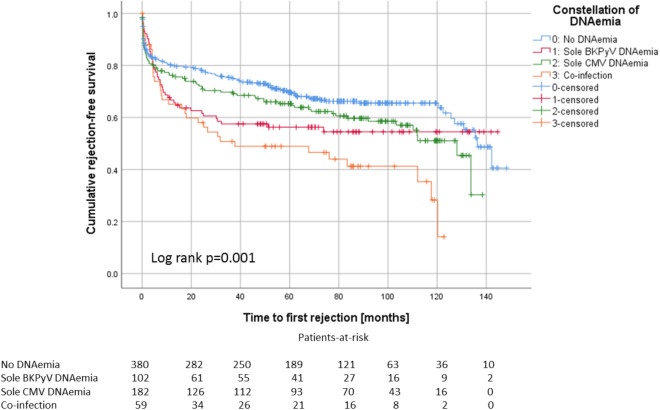
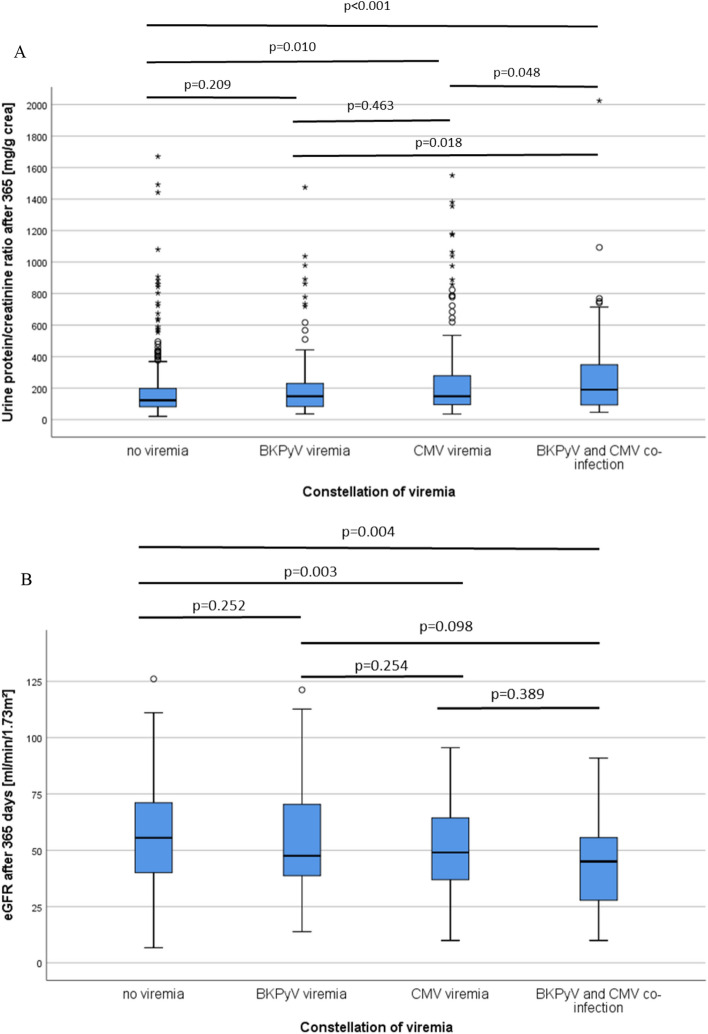
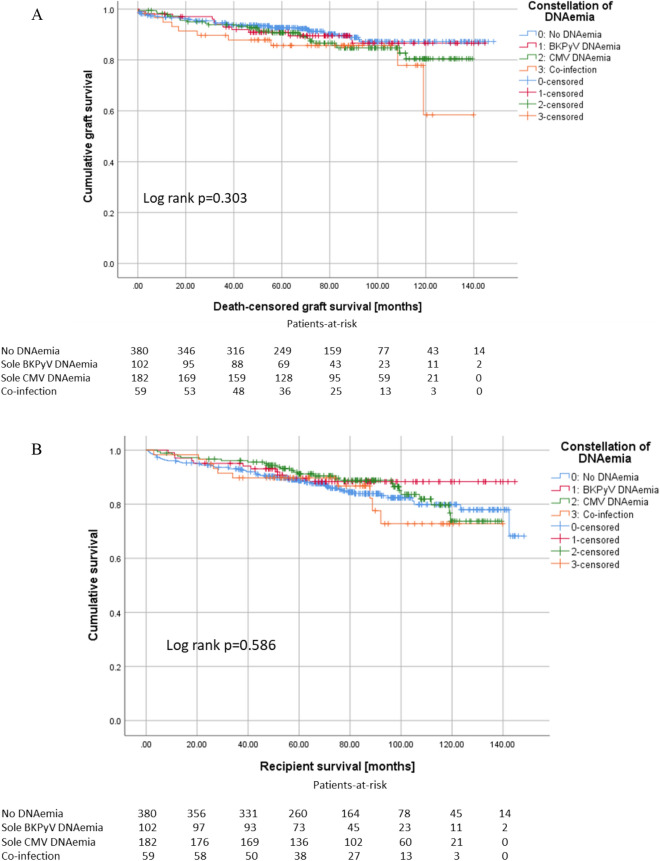
BK polyomavirus (BKPyV) and cytomegalovirus (CMV) are the main viral pathogens affecting the graft and recipient outcome after allogenic kidney transplantation. It has recently been found that infection with both viruses has a greater impact on kidney graft function than a single infection. We retrospectively analyzed a cohort of 723 recipients who received kidney transplantation between 2007 and 2015 after living and postmortal donation for differences in risk and outcome parameters regarding BKPyV (DNAemia) and CMV (CMV DNAemia) co-infection compared to sole viremias and to patients without viremia. Of all kidney allograft recipients in our cohort, 8.2% developed co-infection with BKPyV DNAemia and CMV DNAemia, 15.1% showed BKPyV viremia alone and 25.2% sole CMV DNAemia. Acute rejection was closely linked with co-infection (multivariable analysis, p = 0.001). Despite the fact that the estimated glomerular filtration rate of patients with co-infection was noticeably reduced compared to patients with BKV or CMV infection alone, transplant survival and patient survival were not significantly reduced. Co-infection with BKPyV and CMV in kidney transplanted patients is significantly associated with inferior allograft function. Since co-infection is strongly associated with acute rejection, co-infected individuals should be considered a risk collective.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Hirsch HH, Randhawa PS. BK polyomavirus in solid organ transplantation-Guidelines from the American Society of transplantation infectious diseases community of practice. Clin. Transplant. 2019;33:e13528. - PubMed
