

Methotrexate (MTX) Plus Hydroxychloroquine versus MTX Plus Leflunomide in Patients with MTX-Resistant Active Rheumatoid Arthritis: A 2-Year Cohort Study in Real World
- PMID: 33376379
- PMCID: PMC7755368
- DOI: 10.2147/JIR.S282249
Methotrexate (MTX) Plus Hydroxychloroquine versus MTX Plus Leflunomide in Patients with MTX-Resistant Active Rheumatoid Arthritis: A 2-Year Cohort Study in Real World
Abstract
Purpose: To compare the efficacy, safety, and cost-effectiveness of methotrexate (MTX) plus hydroxychloroquine (HCQ) vs MTX plus leflunomide (LEF) in established rheumatoid arthritis (RA) with inadequate response to MTX monotherapy in a real-world Chinese cohort.
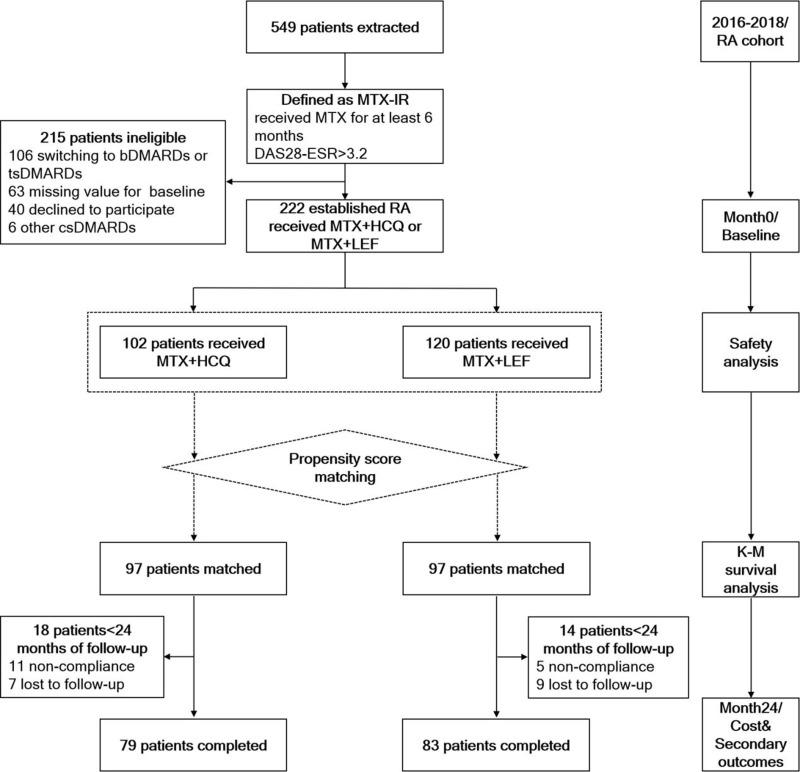
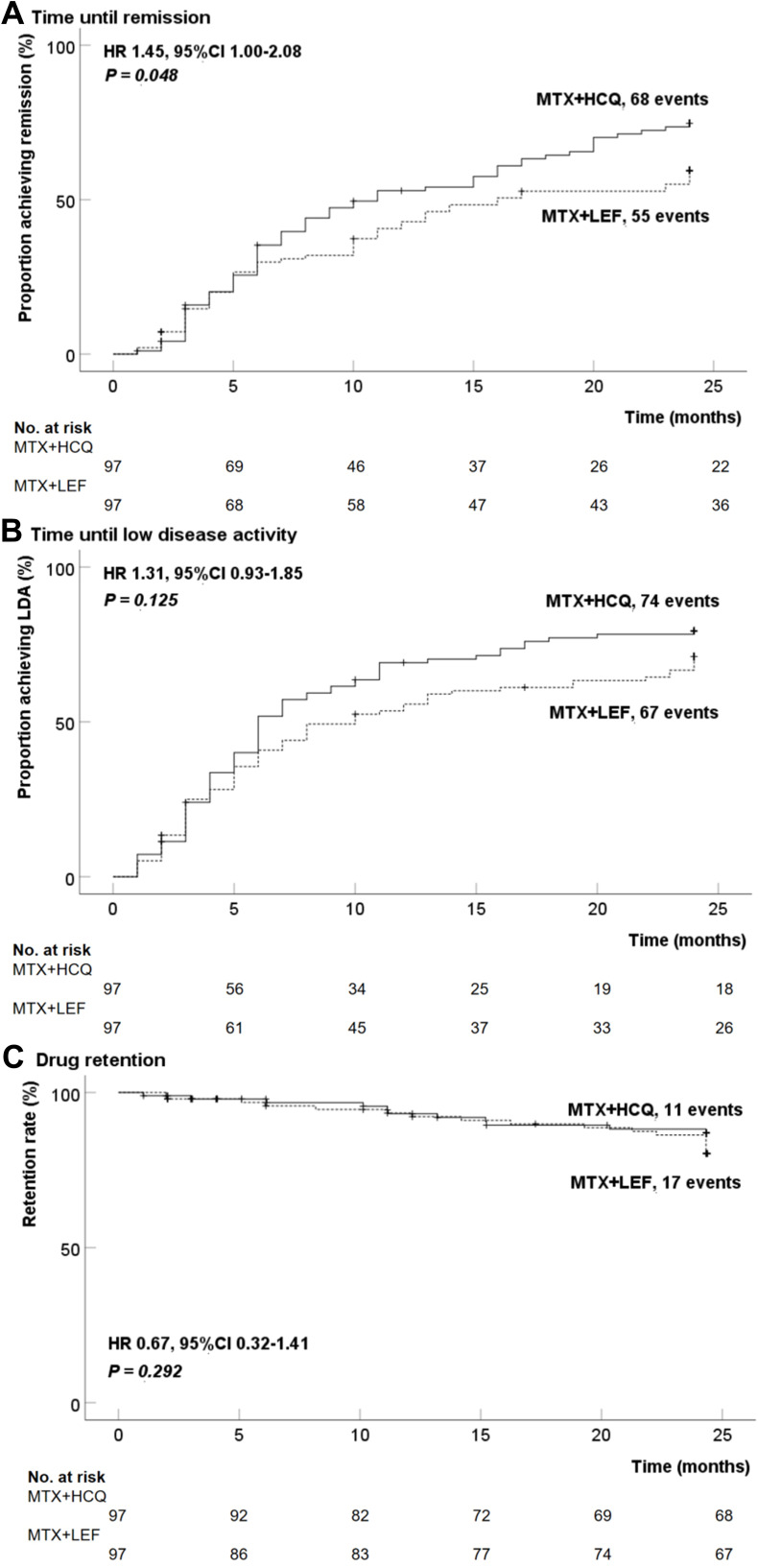
Patients and methods: A prospective RA cohort (n=549) was screened with eligible patients who had inadequate response (disease activity score in 28 joints using erythrocyte sedimentation rate, DAS28-ESR>3.2) to initial MTX monotherapy and subsequently received either MTX+HCQ or MTX+LEF. Propensity score matching (PSM) was applied to adjust the possible baseline confounders between two groups. The primary outcome was the proportion of patients achieving first remission (DAS28-ESR<2.6) during follow-up by log rank test. Secondary outcomes were changes of DAS28, glucocorticoids (GCs) exposure, safety, cost-effectiveness, sustained remission, and low disease activity (LDA) rate after 24-month follow-up.
Results: Overall, 222 eligible patients were subjected to the aforementioned two treatment protocols (MTX+HCQ, n=102; MTX+LEF, n=120). After PSM adjustment, 97 patients in each group were analyzed. A higher remission rate was observed in the MTX+HCQ group than in the MTX+LEF group (70.1% vs 56.7%, P=0.048). The median time to remission was 11 and 16 months in the two groups, respectively. At the endpoint, more patients achieved remission (46.8% vs 32.5%, P=0.063) and maintained sustained LDA in the HCQ group (53.2% vs 38.6%, P=0.062) and also more patients withdrew GCs in this group (32% vs 16.7%, P=0.053) than those in the LEF group. Safety profiles were non-alarming, with no significant difference between the two groups. The incremental cost-effectiveness ratio yielded by MTX+HCQ over MTX+LEF was $1,111.8 per quality-adjusted life-year (QALY), within the cost-effective threshold set as the per capita gross domestic product (GDP) of China.
Conclusion: The MTX+HCQ combination was seemingly superior to MTX+LEF in a real-world cohort of Chinese RA patients with inadequate response to methotrexate monotherapy in respect of the efficacy and cost-effectiveness.
Keywords: cost-effectiveness; efficacy; hydroxychloroquine; leflunomide; methotrexate-resistant; rheumatoid arthritis.
© 2020 Zhang et al.
Conflict of interest statement
The authors declare that they have no conflict of interests.
Figures
References
-
- van Vollenhoven RF, Ernestam S, Geborek P, et al. Addition of infliximab compared with addition of sulfasalazine and hydroxychloroquine to methotrexate in patients with early rheumatoid arthritis (Swefot trial): 1-year results of a randomised trial. Lancet. 2009;374(9688):459–466. doi: 10.1016/s0140-6736(09)60944-2 - DOI - PubMed
-
- Moreland LW, O’Dell JR, Paulus HE, et al. A randomized comparative effectiveness study of oral triple therapy versus etanercept plus methotrexate in early aggressive rheumatoid arthritis: the treatment of early aggressive rheumatoid arthritis trial. Arthritis Rheum. 2012;64(9):2824–2835. doi: 10.1002/art.34498 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
