

A Nomogram Based on Clinicopathologic Features and Preoperative Hematology Parameters to Predict Occult Peritoneal Metastasis of Gastric Cancer: A Single-Center Retrospective Study
- PMID: 33376558
- PMCID: PMC7746455
- DOI: 10.1155/2020/1418978
A Nomogram Based on Clinicopathologic Features and Preoperative Hematology Parameters to Predict Occult Peritoneal Metastasis of Gastric Cancer: A Single-Center Retrospective Study
Abstract
Background: In patients with gastric cancer (GC), peritoneal metastasis is an indication of the end stage and often indicates a poor outcome. The diagnosis of peritoneal metastasis, especially occult peritoneal metastasis (OPM), remains a challenge for surgeons. This study was designed to explore the relationship between OPM and clinicopathological characteristics and preoperative hematological parameters in patients with GC and to develop a nomogram to predict the probability of OPM before surgery.
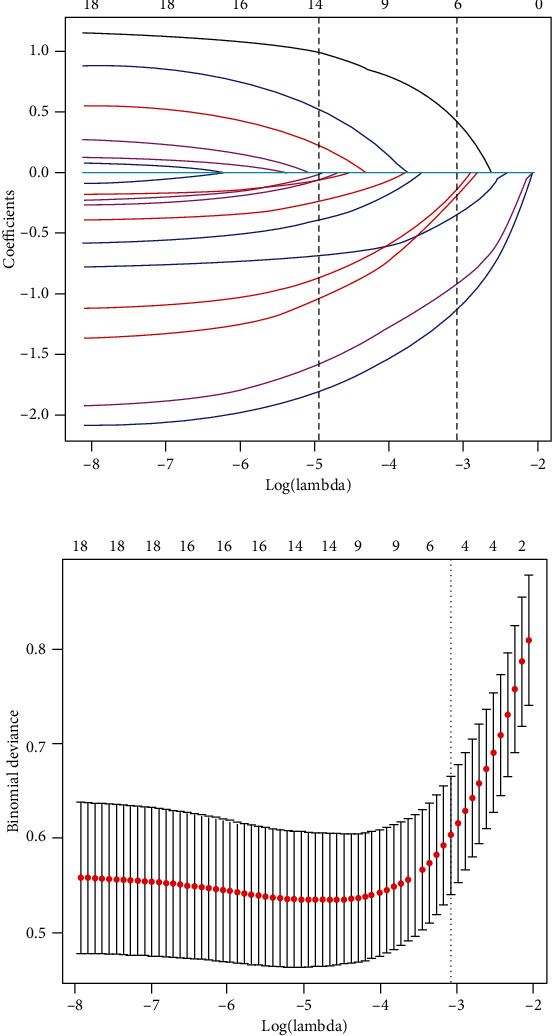
Methods: A total of 672 patients with GC from our center were included, including 583 OPM-negative and 89 OPM-positive patients. These patients were divided into training and validation groups based on when they received treatment. OPM was diagnosed during surgery in patients without any signs of metastasis through imaging examination. Predictive factors were screened by least absolute shrinkage and selection operator logistic regression of all 18 characteristics. The nomogram of OPM was constructed based on these filtered variables. The discriminative and calibration performance of the model were simultaneously evaluated.
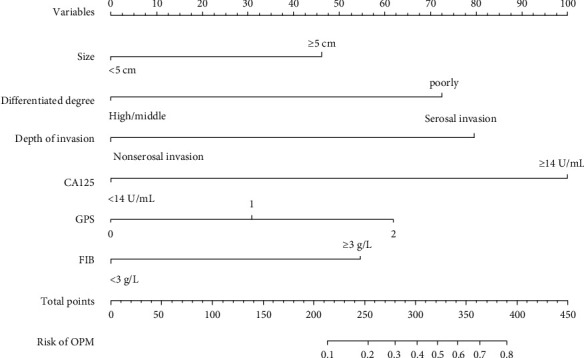
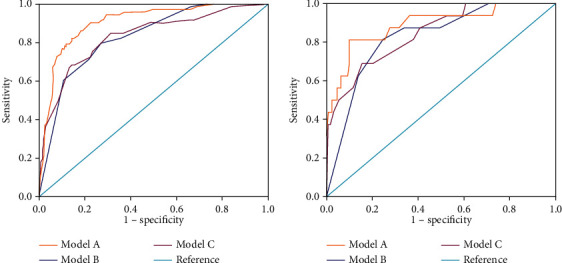
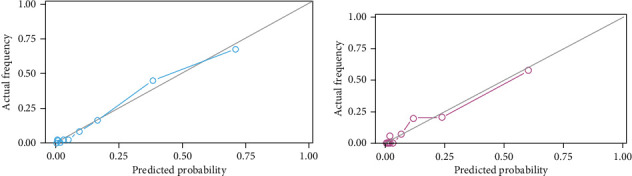
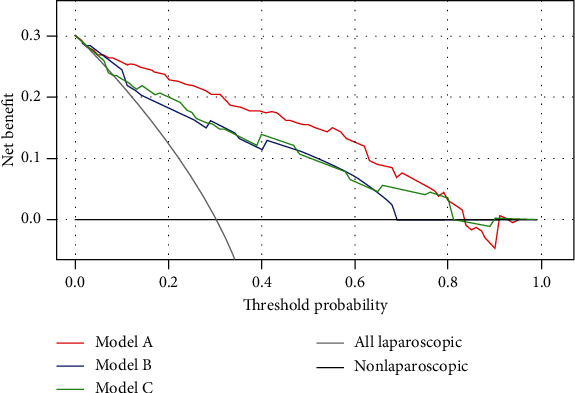
Results: A total of six variables, including tumor size, degree of differentiation, depth of invasion, Glasgow prognosis score, and plasma levels of CA125 and fibrinogen, were selected for integration into the final predictive nomogram. The area under curve (AUC) of the nomogram with six factors was 0.906 (95% confidence interval (CI): 0.872-0.941) and 0.889 (95% CI: 0.795-0.984) in the training and validation groups, respectively. Calibration plots of the nomogram in the two sets revealed a good consistency between predicted and actual probabilities. Decision curve analysis showed that the nomogram had a positive net benefit among all threshold probabilities between 0% and 82%. This nomogram was superior to models incorporating only clinicopathologic or hematologic features.
Conclusion: Both clinicopathological and preoperative hematological parameters are significantly associated with OPM. The nomogram constructed with six factors could be used to calculate the probability of OPM and identify the high-risk population in GC. This may be helpful for early detection of OPM in patients with GC.
Copyright © 2020 Chao Yang et al.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Nakayama I., Chin K., Matsushima T., et al. Retrospective comparison of S-1 plus cisplatin versus S-1 monotherapy for the treatment of advanced gastric cancer patients with positive peritoneal cytology but without gross peritoneal metastasis. International Journal of Clinical Oncology. 2017;22(6):1060–1068. doi: 10.1007/s10147-017-1164-4. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
