

Anticoagulation for Patients with Venous Thromboembolism: When is Extended Treatment Required?
- PMID: 33376944
- PMCID: PMC7758152
- DOI: 10.1055/s-0040-1721735
Anticoagulation for Patients with Venous Thromboembolism: When is Extended Treatment Required?
Abstract
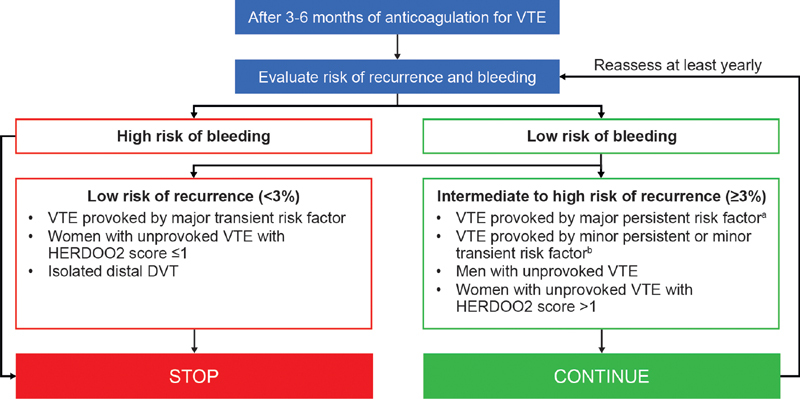
The need for extended venous thromboembolism (VTE) treatment beyond 3 to 6 months is usually determined by balancing the risk of recurrence if treatment is stopped against the risk of bleeding from continuing treatment. The risk of recurrence, and in turn the decision to extend, can be determined through the nature of the index event. Patients with VTE provoked by surgery or trauma (major transient risk factors) are recommended to receive 3 months of anticoagulation therapy because their risk of recurrence is low, whereas patients with VTE provoked by a major persistent risk factor, such as cancer, or those considered to have "unprovoked" VTE, are recommended to receive an extended duration of therapy based on an established high risk of recurrence. Nonetheless, recent evidence and new guidance identify that this approach fails to consider patients with risk factors classed as minor transient (e.g., impaired mobility and pregnancy) or minor persistent (e.g., inflammatory bowel disease and congestive heart disease). Indeed, the risk of recurrence with respect to VTE provoked by minor persistent risk factors has been demonstrated to be not dissimilar to that of VTE without identifiable risk factors. This review provides an overview of the available data on the risk of recurrence according to the underlying cause of VTE, a critical evaluation of evidence from clinical studies on the available anticoagulants for extended VTE treatment, models of risk prediction for recurrent VTE and bleeding, and guidance on how to apply the evidence in practice.
Keywords: anticoagulants; recurrence; risk assessment; risk factors; venous thromboembolism.
The Author(s). This is an open access article published by Thieme under the terms of the Creative Commons Attribution License, permitting unrestricted use, distribution, and reproduction so long as the original work is properly cited. ( https://creativecommons.org/licenses/by/4.0/ ).
Conflict of interest statement
Conflict of interest J.I.W. receives consulting fees from Bayer AG, Boehringer Ingelheim, Bristol Myers Squibb, Daiichi Sankyo, Ionis Pharmaceuticals, Janssen, Johnson & Johnson, Novartis, Pfizer, Portola Pharmaceuticals, and Servier. P.P. receives consulting and lecture fees from Bayer AG, Daiichi Sankyo, Pfizer, and Sanofi. P.V. receives grant support, lecture fees, and fees for serving on advisory boards from Boehringer Ingelheim and LEO Pharma; lecture fees from Bristol Myers Squibb and Pfizer; grant support from Sanofi; lecture fees and fees for serving on advisory boards from Daiichi Sankyo; and fees for serving on an advisory board from Portola Pharmaceuticals.
Figures
References
-
- Martinez C, Cohen A T, Bamber L, Rietbrock S. Epidemiology of first and recurrent venous thromboembolism: a population-based cohort study in patients without active cancer. Thromb Haemost. 2014;112(02):255–263. - PubMed
-
- Kearon C, Akl E A, Ornelas J. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016;149(02):315–352. - PubMed
-
- Key N S, Khorana A A, Kuderer N M. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2020;38(05):496–520. - PubMed
-
- International Initiative on Thrombosis and Cancer (ITAC) advisory panel . Farge D, Frere C, Connors J M. 2019 international clinical practice guidelines for the treatment and prophylaxis of venous thromboembolism in patients with cancer. Lancet Oncol. 2019;20(10):e566–e581. - PubMed
Publication types
LinkOut - more resources
Full Text Sources