

Establishing two principal dimensions of cognitive variation in logopenic progressive aphasia
- PMID: 33376980
- PMCID: PMC7750924
- DOI: 10.1093/braincomms/fcaa125
Establishing two principal dimensions of cognitive variation in logopenic progressive aphasia
Abstract
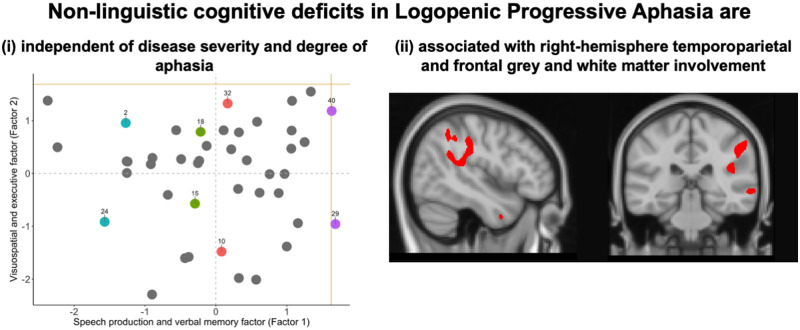
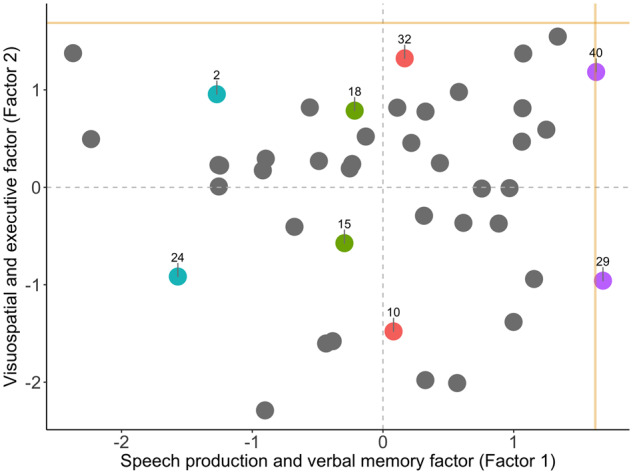
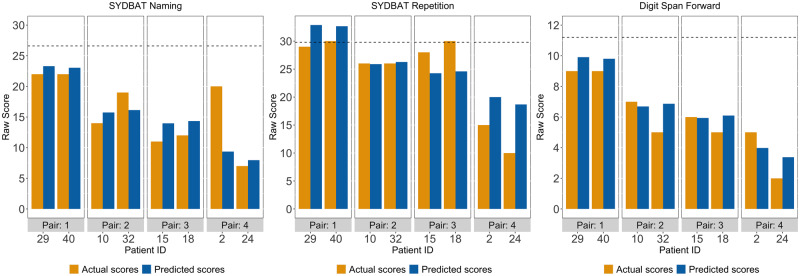
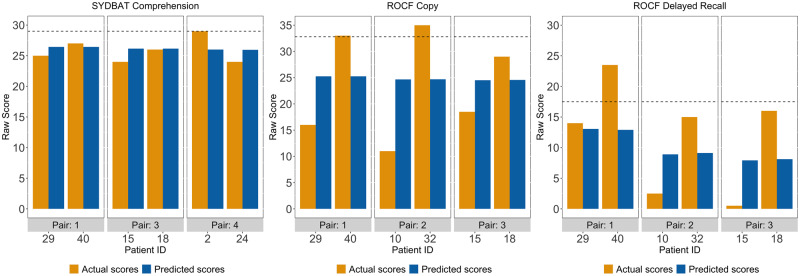
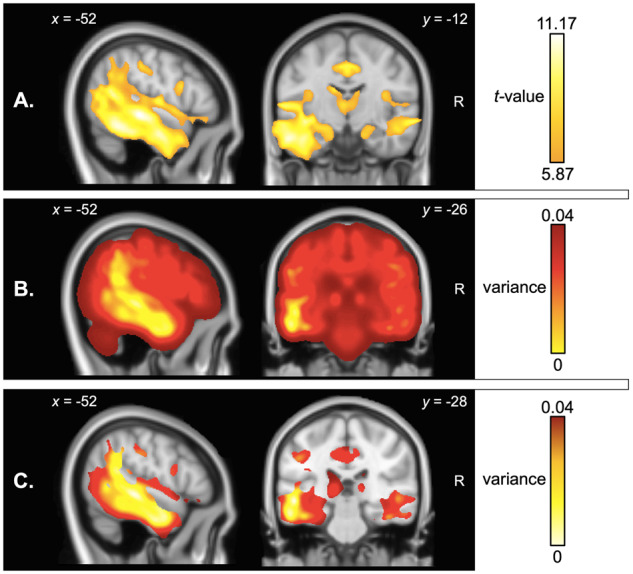
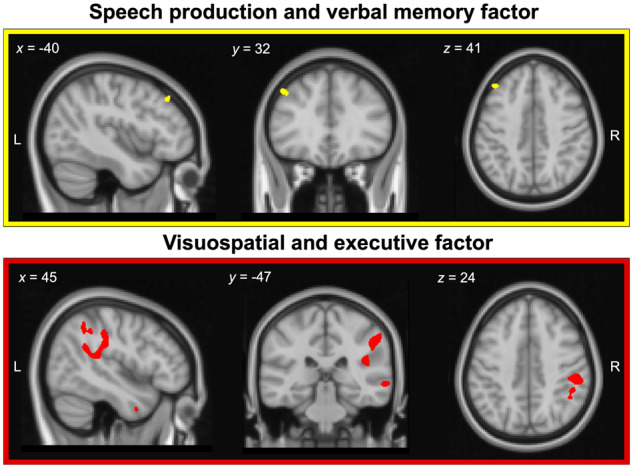
Logopenic progressive aphasia is a neurodegenerative syndrome characterized by sentence repetition and naming difficulties arising from left-lateralized temporoparietal atrophy. Clinical descriptions of logopenic progressive aphasia largely concentrate on profiling language deficits, however, accumulating evidence points to the presence of cognitive deficits even on tasks with minimal language demands. Although non-linguistic cognitive deficits in logopenic progressive aphasia are thought to scale with disease severity, patients at discrete stages of language dysfunction display overlapping cognitive profiles, suggesting individual-level variation in cognitive performance, independent of primary language dysfunction. To address this issue, we used principal component analysis to decompose the individual-level variation in cognitive performance in 43 well-characterized logopenic progressive aphasia patients who underwent multi-domain neuropsychological assessments and structural neuroimaging. The principal component analysis solution revealed the presence of two, statistically independent factors, providing stable and clinically intuitive explanations for the majority of variance in cognitive performance in the syndrome. Factor 1 reflected 'speech production and verbal memory' deficits which typify logopenic progressive aphasia. Systematic variations were also confirmed on a second, orthogonal factor mainly comprising visuospatial and executive processes. Adopting a case-comparison approach, we further demonstrate that pairs of patients with comparable Factor 1 scores, regardless of their severity, diverge considerably on visuo-executive test performance, underscoring the inter-individual variability in cognitive profiles in comparably 'logopenic' patients. Whole-brain voxel-based morphometry analyses revealed that speech production and verbal memory factor scores correlated with left middle frontal gyrus, while visuospatial and executive factor scores were associated with grey matter intensity of right-lateralized temporoparietal, middle frontal regions and their underlying white matter connectivity. Importantly, logopenic progressive aphasia patients with poorer visuospatial and executive factor scores demonstrated greater right-lateralized temporoparietal and frontal atrophy. Our findings demonstrate the inherent variation in cognitive performance at an individual- and group-level in logopenic progressive aphasia, suggesting the presence of a genuine co-occurring cognitive impairment that is statistically independent of language function and disease severity.
Keywords: executive functioning; language; primary progressive aphasia; principal component analysis; visuospatial functioning.
© The Author(s) (2020). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures
References
-
- Aron AR, Robbins TW, Poldrack RA. Inhibition and the right inferior frontal cortex. Trends Cogn Sci 2004; 8: 170–7. - PubMed
-
- Benjamini Y, Hochberg Y. Controlling the false discovery rate - a practical and powerful approach to multiple testing. J R Stat Soc B 1995; 57: 289–300.
Grants and funding
LinkOut - more resources
Full Text Sources