

Frequent neurocognitive deficits after recovery from mild COVID-19
- PMID: 33376990
- PMCID: PMC7717144
- DOI: 10.1093/braincomms/fcaa205
Frequent neurocognitive deficits after recovery from mild COVID-19
Abstract
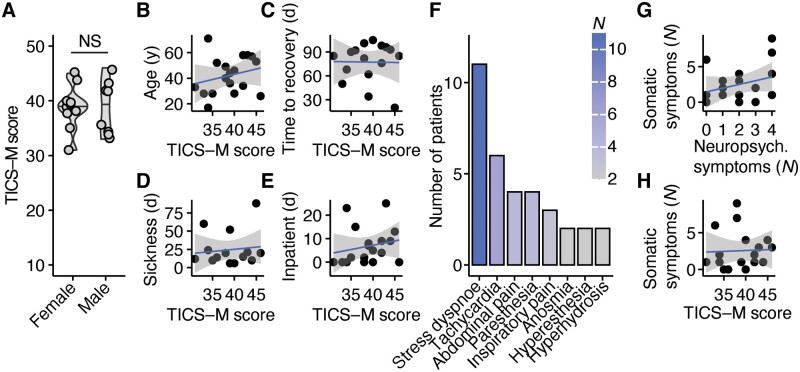
Neuropsychiatric complications associated with coronavirus disease 2019 caused by the Coronavirus SARS-CoV-2 (COVID-19) are increasingly appreciated. While most studies have focussed on severely affected individuals during acute infection, it remains unclear whether mild COVID-19 results in neurocognitive deficits in young patients. Here, we established a screening approach to detect cognitive deficiencies in post-COVID-19 patients. In this cross-sectional study, we recruited 18 mostly young patients 20-105 days (median, 85 days) after recovery from mild to moderate disease who visited our outpatient clinic for post-COVID-19 care. Notably, 14 (78%) patients reported sustained mild cognitive deficits and performed worse in the Modified Telephone Interview for Cognitive Status screening test for mild cognitive impairment compared to 10 age-matched healthy controls. While short-term memory, attention and concentration were particularly affected by COVID-19, screening results did not correlate with hospitalization, treatment, viremia or acute inflammation. Additionally, Modified Telephone Interview for Cognitive Status scores did not correlate with depressed mood or fatigue. In two severely affected patients, we excluded structural or other inflammatory causes by magnetic resonance imaging, serum and cerebrospinal fluid analyses. Together, our results demonstrate that sustained sub-clinical cognitive impairments might be a common complication after recovery from COVID-19 in young adults, regardless of clinical course that were unmasked by our diagnostic approach.
Keywords: COVID-19; neurocognitive deficits; neurocognitive screenings; post-COVID-19.
© The Author(s) (2020). Published by Oxford University Press on behalf of the Guarantors of Brain.
Figures



References
-
- De Jager CA, Budge MM, Clarke R.. Utility of TICS-M for the assessment of cognitive function in older adults. Int J Geriatr Psychiatry 2003; 18: 318–24. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous