

Inclusion of the Acetabular Labrum Reduces Simulated Range of Motion of the Hip Compared With Bone Contact Models
- PMID: 33376992
- PMCID: PMC7754612
- DOI: 10.1016/j.asmr.2020.07.014
Inclusion of the Acetabular Labrum Reduces Simulated Range of Motion of the Hip Compared With Bone Contact Models
Abstract
Purpose: To determine whether inclusion of the acetabular labrum affects the maximum range of motion (ROM) during simulation of the flexion-adduction-internal rotation impingement examination.
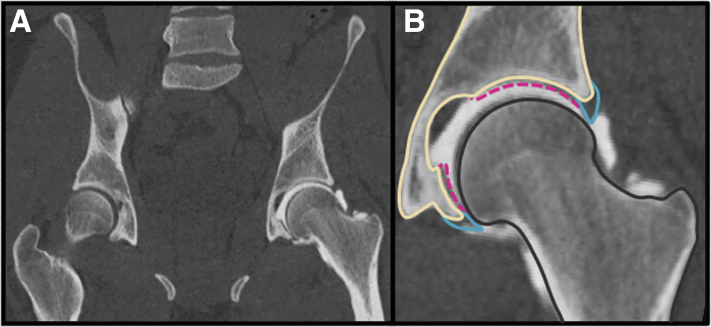
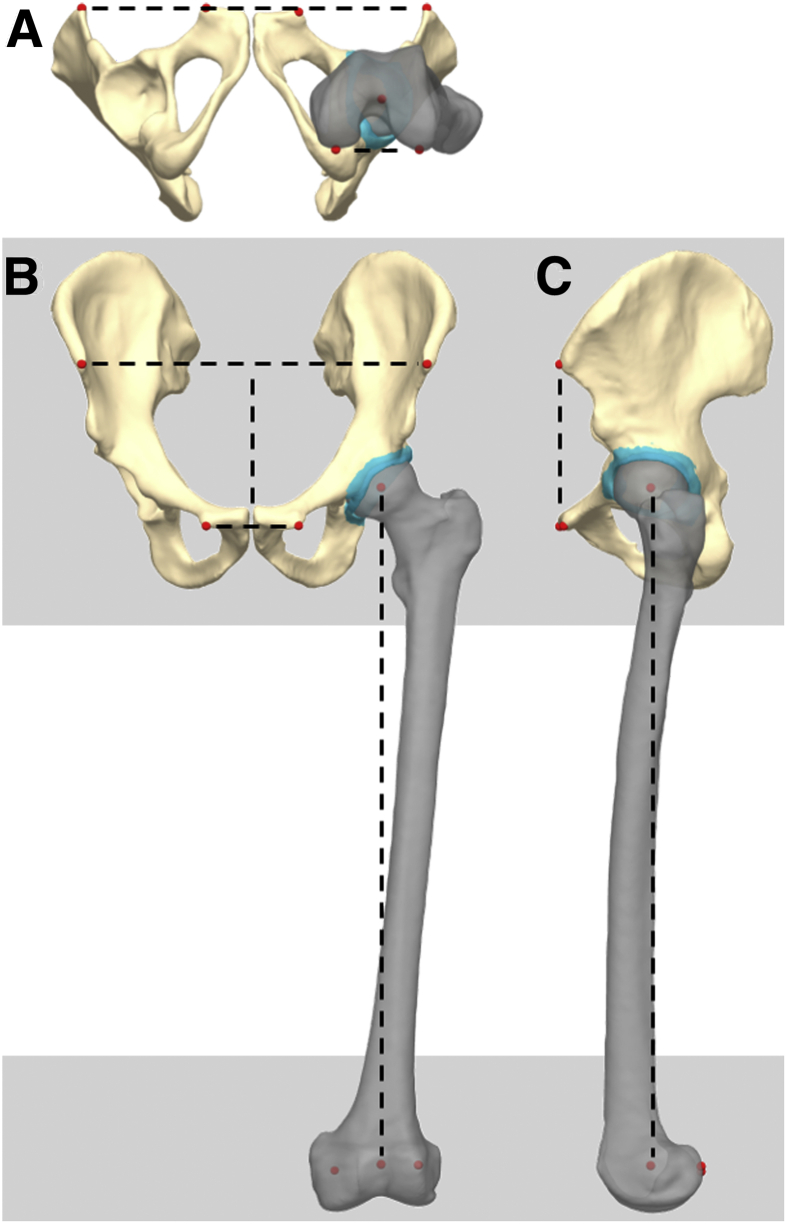
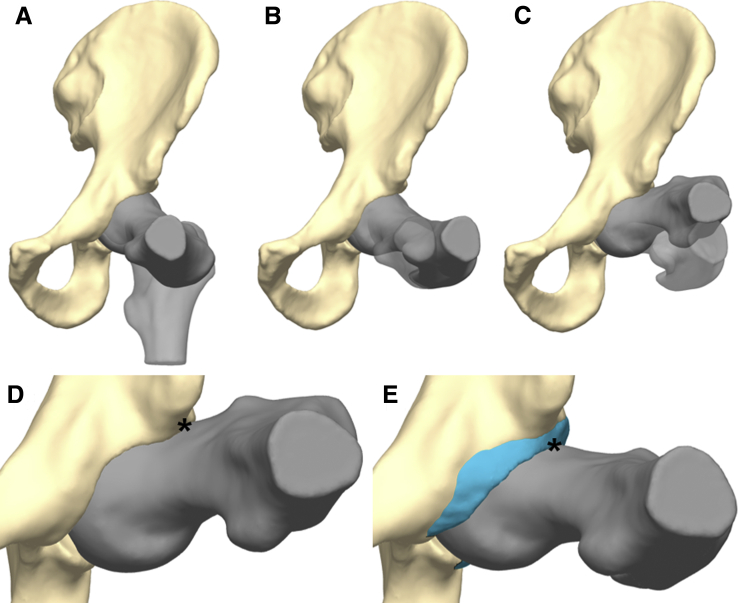
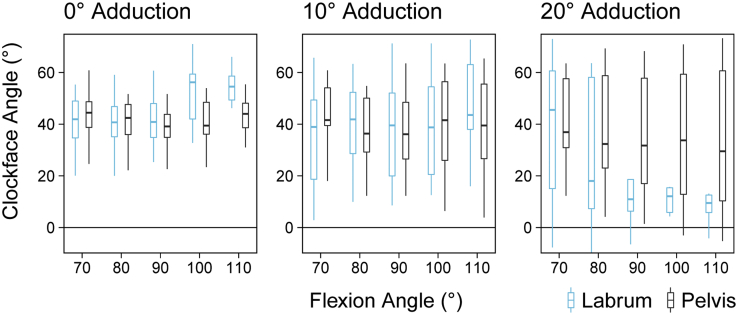
Methods: Three-dimensional surface reconstructions of the femur, hemi-pelvis, and labrum from computed tomography arthrography images of 19 participants were used to simulate maximum ROM during the flexion-adduction-internal rotation examination. Simulations were conducted for positions between 70° and 110° flexion and 0° and 20° adduction at 10° increments to measure maximum internal rotation and the position of contact between the femur and acetabular rim (bone-to-bone) or the femur and labrum (bone-to-labrum). Internal rotation angles and clock-face position values were compared between the 2 contact scenarios for each position.
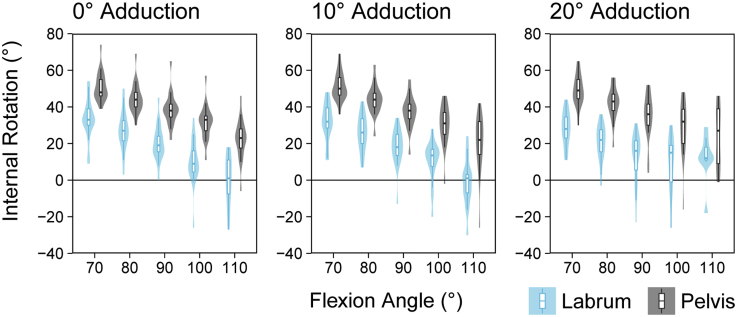
Results: The ROM in the bone-to-labrum contact model was significantly less than that of the bone-to-bone contact model for all evaluated positions (P ≤ .001, except at 110° flexion and 20° adduction, P = .114). The inclusion of the labrum reduced internal rotation by a median [interquartile range] of 18 [15, 25]° while altering the position of contact on the acetabular clock-face by -0:01 [-0:27, 0:16]. The variability in contact location for the bone-to-labrum contact scenario was nearly double that of the bone-to-bone contact scenario, as indicated by the interquartile range.
Conclusions: Inclusion of the anatomy of the acetabular labrum in collision models used to simulate impingement examinations reduced the internal rotation ROM by approximately 20° and increased variability in the location of contact relative to the acetabular rim.
Clinical relevance: While standard bone-to-bone contact ROM simulations may be informative with respect to the relative change in ROM based on a surgical intervention (e.g., pre- and post-osteochondroplasty for cam-type femoroacetabular impingement), they may not accurately represent the clinical ROM of the joint or the kinematic position at which damage may occur due to shape mismatch between the femur and acetabulum.
© 2020 by the Arthroscopy Association of North America. Published by Elsevier Inc.
Figures
References
-
- Ganz R., Parvizi J., Beck M., Leunig M., Notzli H., Siebenrock K.A. Femoroacetabular impingement: A cause for osteoarthritis of the hip. Clin Orthop Rel Res. 2003:112–120. - PubMed
-
- Klaue K., Durnin C.W., Ganz R. The acetabular rim syndrome. A clinical presentation of dysplasia of the hip. J Bone Joint Surg Br. 1991;73:423–429. - PubMed
-
- Audenaert E.A., Mahieu P., Pattyn C. Three-dimensional assessment of cam engagement in femoroacetabular impingement. Arthroscopy. 2011;27:167–171. - PubMed
-
- Bedi A., Dolan M., Magennis E., Lipman J., Buly R., Kelly B.T. Computer-assisted modeling of osseous impingement and resection in femoroacetabular impingement. Arthroscopy. 2012;28:204–210. - PubMed
-
- Hamada H., Takao M., Nakahara I., Sakai T., Nishii T., Sugano N. Hip range-of-motion (ROM) is less than normal after rotational acetabular osteotomy for developmental dysplasia of the hip: A simulated ROM analysis. J Orthop Res. 2016;34:217–223. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
