

Clinical implications of plasma ctDNA features and dynamics in gastric cancer treated with HER2-targeted therapies
- PMID: 33377634
- PMCID: PMC7737756
- DOI: 10.1002/ctm2.254
Clinical implications of plasma ctDNA features and dynamics in gastric cancer treated with HER2-targeted therapies
Abstract
Background: Gastric cancer (GC) is confronted with limited options for precision medicine. Human epidermal growth factor receptor 2 (HER2) is the principal druggable target of GC, yet proper biomarkers for response/resistance prediction remain unveiled.
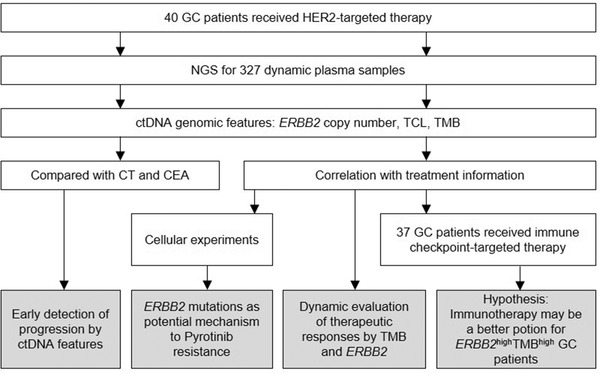
Methods: From 40 GC patients received HER2-targeted therapy, a total of 327 peripheral blood plasma specimens was collected including baseline and treatment time points. Circulating tumor DNA (ctDNA) was extracted and sequenced with a target panel of 425 genes. Experimental validation of resistant mutations was carried out in NIH-3T3 cell line.
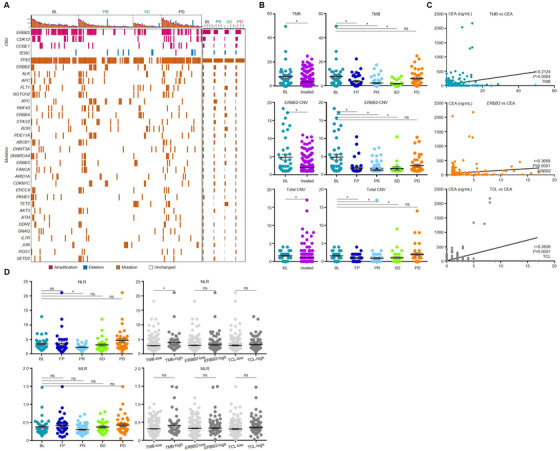
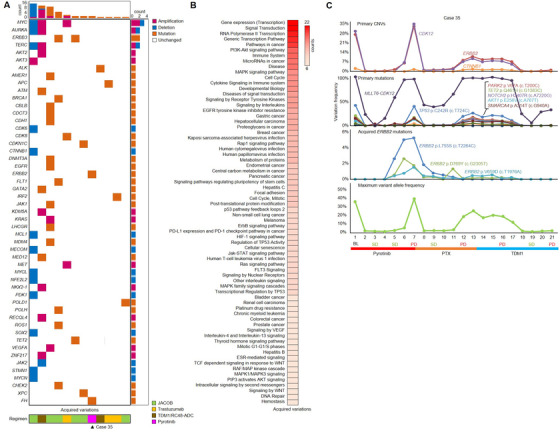
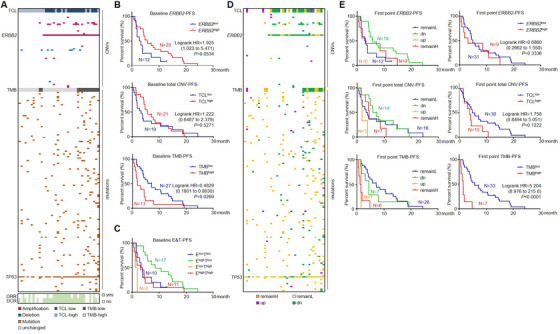
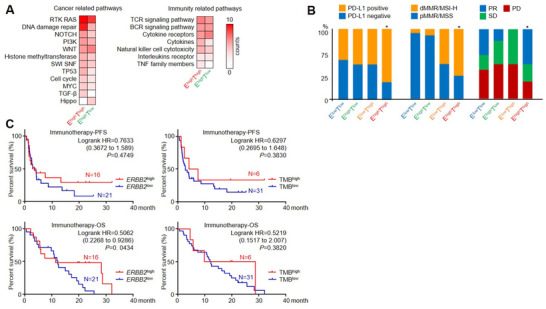
Results: Genomic features, including ERBB2 copy number variation (CNV), total copy number load, and tumor mutation burdens (TMBs), dynamically changed along with the treatment process and correlated with disease progression. Plasma ctDNA-based diagnosis was more sensitive than conventional computed tomography scanning in 40% of investigated patients, gaining additional time for clinical management. Compared to baseline, new gene alterations were emerged in 12 patients who developed drug resistance during treatment. ERBB2 mutations potentially related to Pyrotinib resistance were identified in plasma ctDNA of one patient and functional analysis of their downstream signaling pathways was carried out in NIH-3T3 cell line. TMB exhibited more power than ERBB2 CNV in predicting treatment responses and prognosis for HER2-targeted therapy in GC patients. Interestingly, survival analysis indicated that patients harboring both HER2 (ERBB2) positivity and high TMB might gain more therapeutic benefits from immune checkpoint inhibitors instead of HER2-targeted regimens that required further studies and validations CONCLUSIONS: Our work showed that the dynamic surveillance of plasma ctDNA genomic features provided instructive information for the precision medication of GC patients.
Keywords: ERBB2 copy number; HER2-targeted therapy; TMB; gastric cancer; immunotherapy; liquid biopsy.
© 2020 The Authors. Clinical and Translational Medicine published by John Wiley & Sons Australia, Ltd on behalf of Shanghai Institute of Clinical Bioinformatics.
Conflict of interest statement
Ruoying Yu and Xiaoxi Chen are the employees of Geneseeq Technology Inc Canada. Tingting Sun and Yang Shao are the employee of Nanjing Geneseeq Technology Inc. The remaining authors have no conflicts of interest to declare.
Figures

References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2020. CA Cancer J. Clin. 2020;70(1):7‐30. - PubMed
-
- Van Cutsem E, Sagaert X, Topal B, Haustermans K, Prenen H. Gastric cancer. Lancet. 2016;388(10060):2654‐2664. - PubMed
-
- Dagogo‐Jack I, Shaw AT. Tumour heterogeneity and resistance to cancer therapies. Nat Rev Clin Oncol. 2018;15(2):81‐94. - PubMed
-
- Kurokawa Y, Matsuura N, Kimura Y, et al. Multicenter large‐scale study of prognostic impact of HER2 expression in patients with resectable gastric cancer. Gastric Cancer. 2015;18(4):691‐697. - PubMed
Grants and funding
- 2018YFC1313304/National Key Research and Development Program of China
- 81802327/National Natural Science Foundation of China
- 81872341/National Natural Science Foundation of China
- 91959205/Major Program of National Natural Science Foundation of China
- 2020-1-1022/Capital's Funds for Health Improvement and Research
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous