

Management of primary sclerosing cholangitis and its complications: an algorithmic approach
- PMID: 33377990
- PMCID: PMC7886831
- DOI: 10.1007/s12072-020-10118-x
Management of primary sclerosing cholangitis and its complications: an algorithmic approach
Abstract
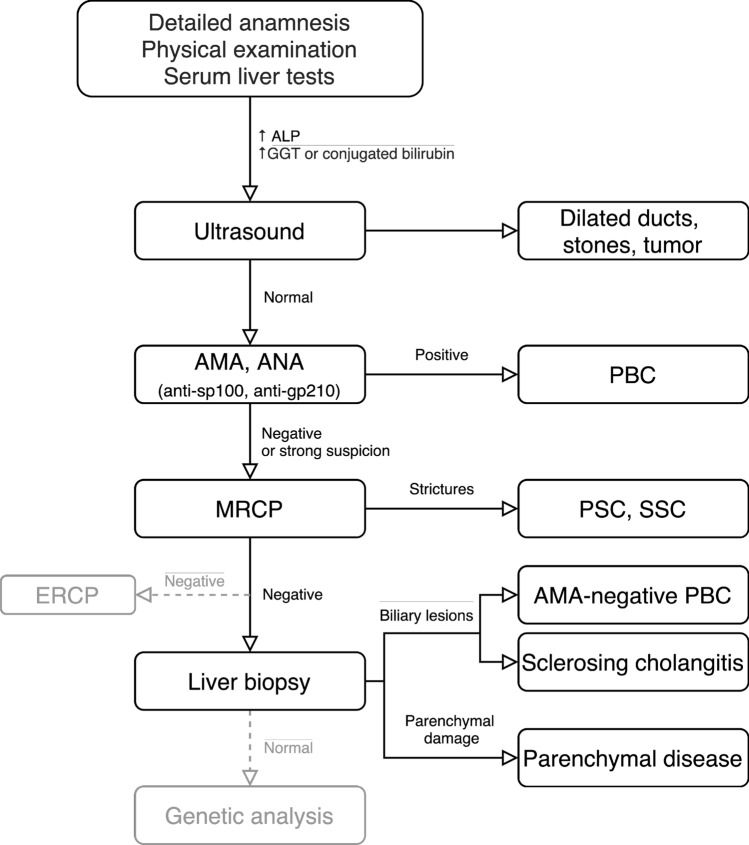
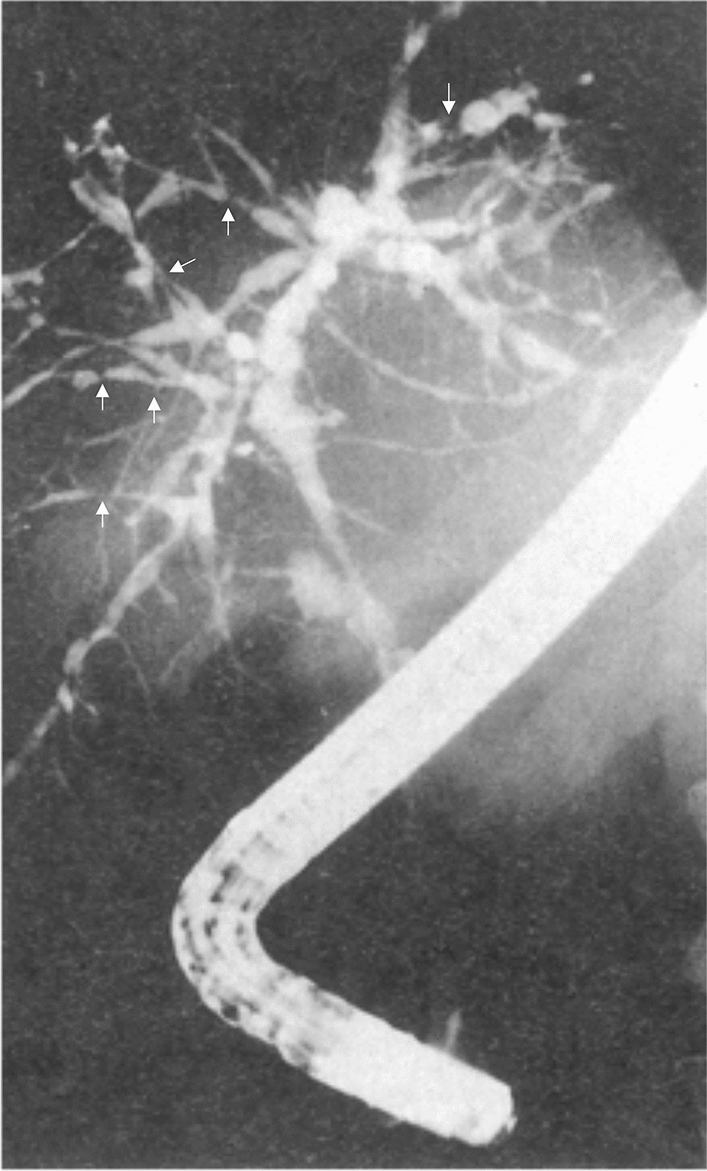
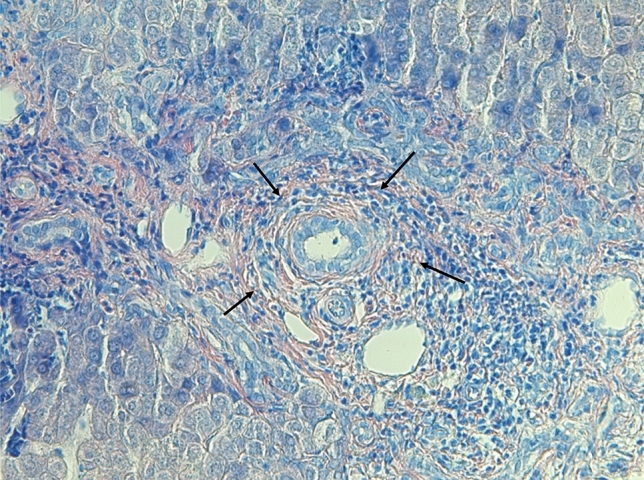
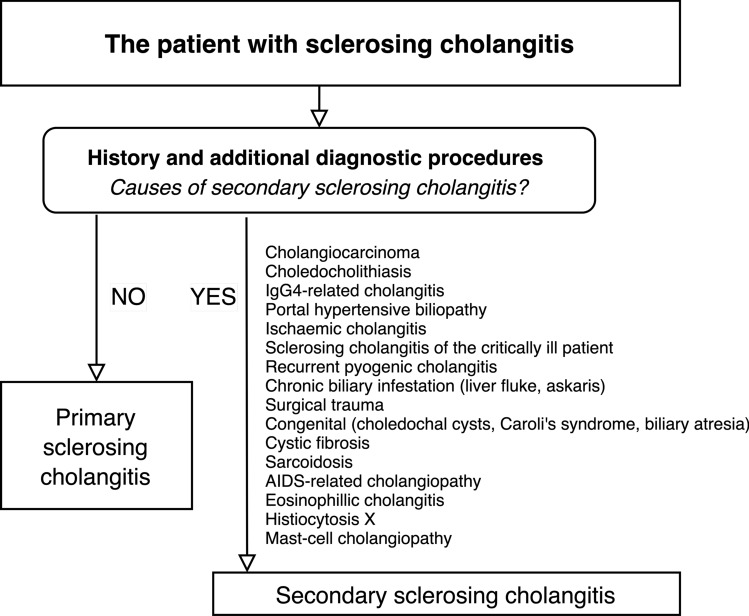
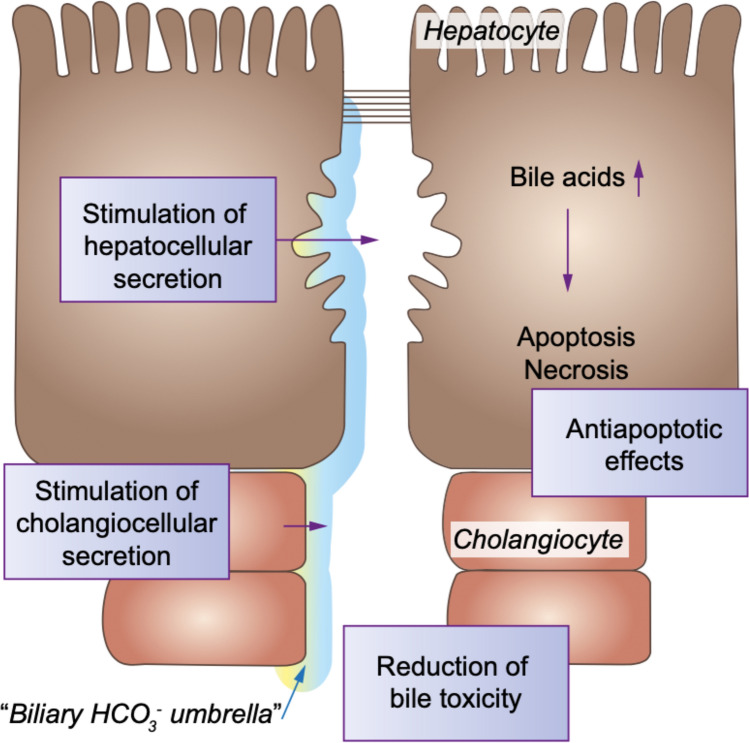
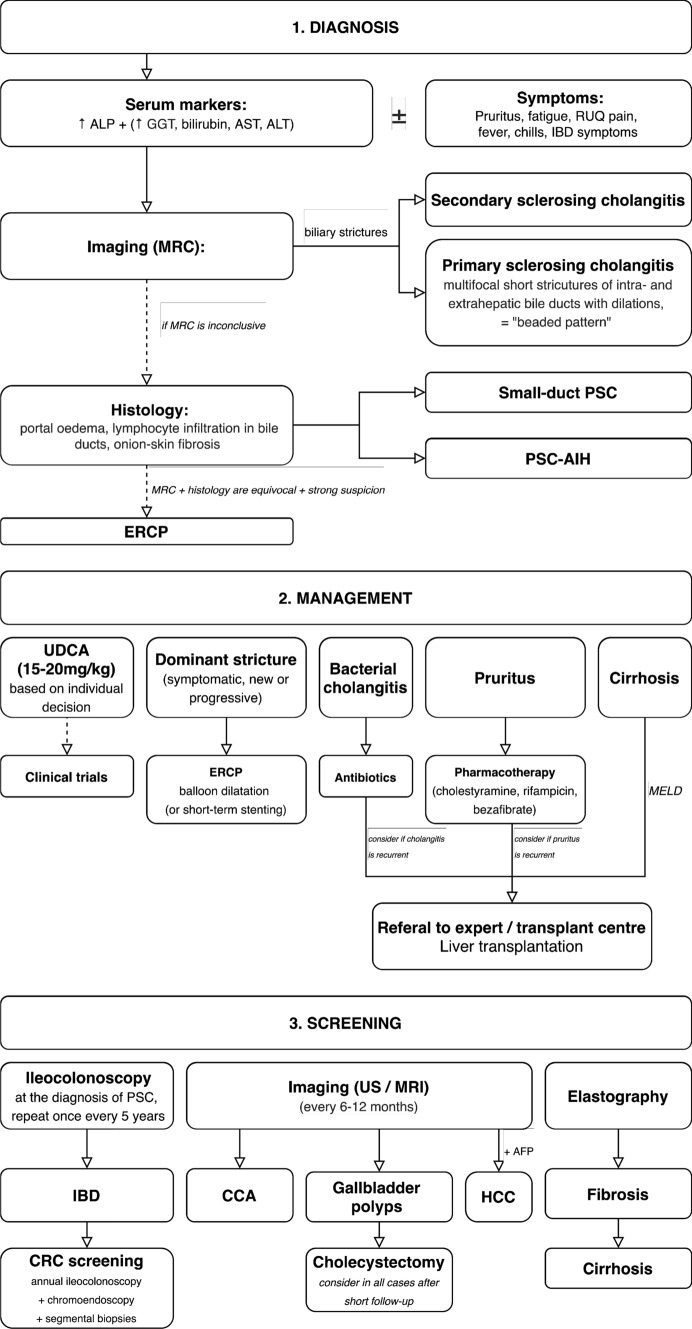
Primary sclerosing cholangitis (PSC) is a rare cholestatic liver disease, characterized by multiple strictures and dilatations of the intra- and extrahepatic bile ducts, leading to progressive liver fibrosis, in 10-15% cholangiocarcinoma, and ultimately end-stage liver disease. The pathogenesis is poorly understood, but (epi-)genetic factors, mechanisms of innate and adaptive immunity, toxic effects of hydrophobic bile acids, and possibly intestinal dysbiosis appear to be involved. The strong link with inflammatory bowel disease (IBD) is associated with a markedly enhanced risk of colorectal cancer which next to cholangiocarcinoma represents the most serious diagnostic challenge in long-term PSC management. Despite extensive research, no medical treatment has been proven so far to prolong the time to liver transplantation (LTx), which remains the effective treatment in late-stage disease. Recurrence of PSC after LTx is observed in up to 20% of patients. Here, we briefly summarize actual views on PSC pathogenesis and provide an algorithmic approach to diagnostic procedures and recommendations for the management of PSC and its complications. We describe promising treatment options subject to current clinical trials.
Keywords: Bezafibrate; Bile acids; Cholangiocarcinoma; Cholestasis; FXR; Liver transplantation; Obeticholic acid; Primary sclerosing cholangitis; Pruritus; Ursodeoxycholic acid.
Conflict of interest statement
MP received a mobility grant from the Erasmus + Programme. UB received grant support via AMC Foundation from a South-African PSC Patient Foundation, grant support via Amsterdam UMC for investigator-initiated studies by Dr. Falk Pharma, Freiburg (Germany), and Intercept, San Diego, CA (USA) and lecture fees from Abbvie, Falk Foundation, Gilead, Intercept.
Figures
References
-
- Chapman MH, Webster GJM, Bannoo S, Johnson GJ, Wittmann J, Pereira SP. Cholangiocarcinoma and dominant strictures in patients with primary sclerosing cholangitis: a 25-year single-centre experience. Eur J Gastroenterol Hepatol. 2012;24(9):1051–1058. doi: 10.1097/MEG.0b013e3283554bbf. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
