The efficacy of ultrasound-guided erector spinae plane block after mastectomy and immediate breast reconstruction with a tissue expander: a randomized clinical trial
- PMID: 33380573
- PMCID: PMC7783852
- DOI: 10.3344/kjp.2021.34.1.106
The efficacy of ultrasound-guided erector spinae plane block after mastectomy and immediate breast reconstruction with a tissue expander: a randomized clinical trial
Abstract
Background: We aimed to investigate the analgesic efficacy of an erector spinae plane block (ESPB) in immediate breast reconstruction (IBR) with a tissue expander.
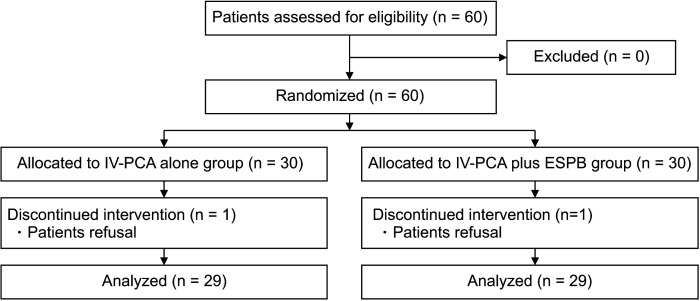
Methods: Adult women undergoing IBR with a tissue expander after mastectomy were randomly assigned to either intravenous patient-controlled analgesia (IV-PCA) alone (group P) or IV-PCA plus ESPB (group E). The primary outcome was the total amount of opioid consumption during 24 hours postoperatively between the two groups. Secondary outcomes were patient satisfaction, pain score at rest and on shoulder movement using numerical rating scale, incidences of postoperative nausea and vomiting (PONV), and a short form of the brief pain inventory (BPI-SF) at 3 and 6 months after surgery between the groups.
Results: Fifty eight patients completed the study. At 24 hours postoperatively, total opioid consumption was significantly less in group E than in group P (285.0 ± 92.0, 95% confidence interval [CI]: 250.1 to 320.0 vs. 223.2 ± 83.4, 95% CI: 191.5 to 254.9, P = 0.005). Intraoperative and cumulative PCA fentanyl consumption at 3, 6, 9, and 24 hours were also less in group E than in group P (P = 0.004, P = 0.048, P = 0.020, P = 0.036, and P < 0.001, respectively). Patient satisfaction was higher in group E (6.9 ± 1.8 vs. 7.8 ± 1.4, P = 0.042). The incidences of PONV was similar.
Conclusions: The ESPB decreased postoperative opioid consumption and increased patient satisfaction without significant complications after IBR with a tissue expander after mastectomy.
Keywords: Analgesia; Breast Implants; Breast Neoplasms; Interventional; Mastectomy; Nerve Block; Pain; Patient Satisfaction; Postoperative; Reconstructive Surgical Procedures; Tissue Expansion Devices; Ultrasonography.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
LinkOut - more resources
Full Text Sources
Other Literature Sources