

Chest radiography of contemporary trans-catheter cardiovascular devices: a pictorial essay
- PMID: 33381431
- PMCID: PMC7758755
- DOI: 10.21037/cdt-20-617
Chest radiography of contemporary trans-catheter cardiovascular devices: a pictorial essay
Abstract
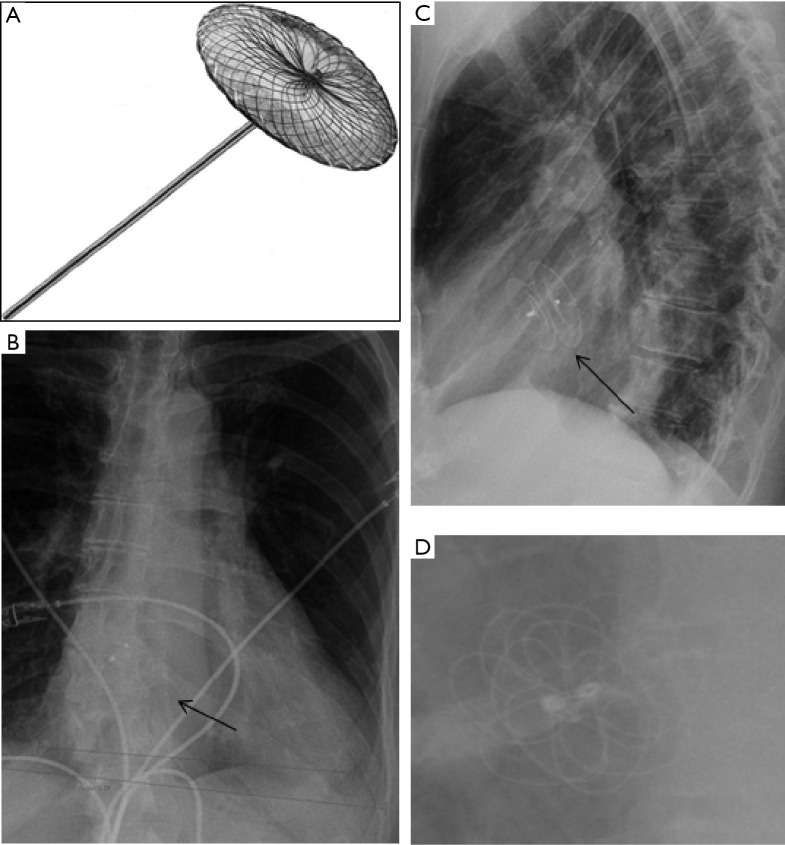
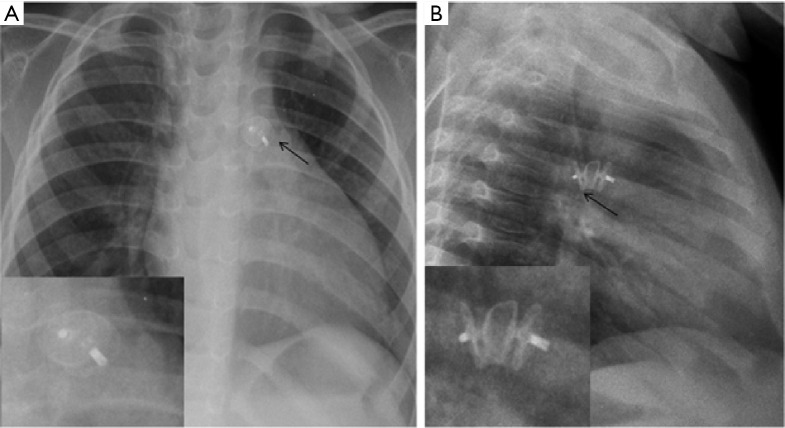
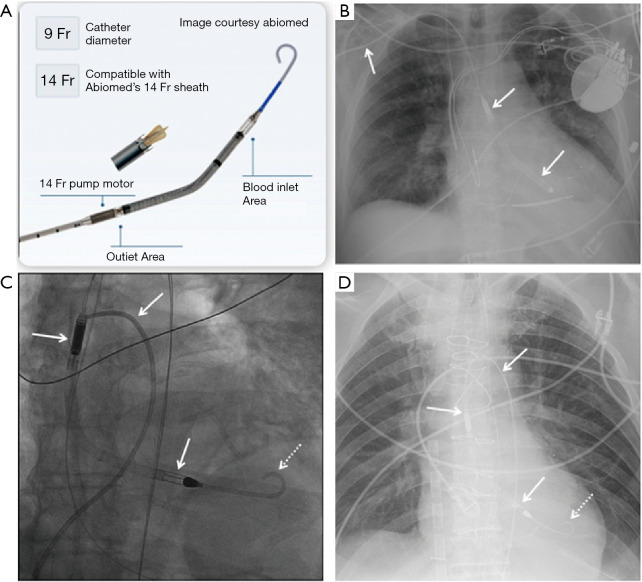
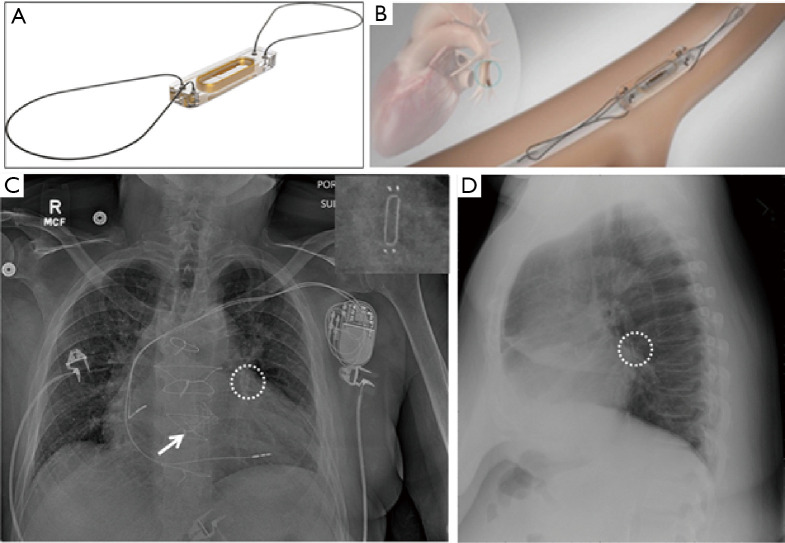
There is a plethora of cardiovascular devices used for therapy and monitoring, and newer devices are being introduced constantly. As a result of advancement of medical technology and rapid development of such technology to address unmet needs across cardiovascular care, multiple conditions which were previously treated surgically or with medications now benefit from trans-catheter device-based evaluation and management. Moreover, innovation to existing technology has transformed the structural design of many traditional cardiovascular devices, making them safer and enabling easier deployment within the chest (catheter-based versus surgical). A post-procedure chest radiography (CXR) is often the first routine imaging test ordered in these patients. A CXR is a relatively inexpensive and noninvasive imaging tool, which can be obtained at the patient's bedside if needed. Commonly implanted cardiovascular devices can be quite easily checked for appropriate positioning on routine CXRs. Potential complications associated with mal-positioning of such devices may be life-threatening. Such complications often manifest early on CXRs and may not be readily apparent on clinical examination. Prompt recognition of such abnormal radiographic appearances is critical for timely diagnosis and effective management. Clinicians need to be familiar with new devices in order to assess proper placement and identify complications related to mal-positioning. This pictorial essay aims to describe the radiologic appearances of contemporary cardiovascular devices, review indications for their usage and potential complications, and discuss magnetic resonance imaging (MRI) compatibility.
Keywords: Cardiovascular devices; chest radiography (CXR); trans-catheter.
2020 Cardiovascular Diagnosis and Therapy. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at http://dx.doi.org/10.21037/cdt-20-617). The authors have no conflicts of interest to declare.
Figures












Similar articles
-
Uncommon Iatrogenic Devices Seen on Chest Radiographs.Indian J Radiol Imaging. 2021 Jan;31(1):172-184. doi: 10.1055/s-0041-1729487. Epub 2021 May 31. Indian J Radiol Imaging. 2021. PMID: 34316125 Free PMC article.
-
Chest radiography in the ICU.Clin Imaging. 1997 Mar-Apr;21(2):90-103. doi: 10.1016/0899-7071(95)00097-6. Clin Imaging. 1997. PMID: 9095383 Review.
-
Radiographic Review of Current Therapeutic and Monitoring Devices in the Chest.Radiographics. 2018 Jul-Aug;38(4):1027-1045. doi: 10.1148/rg.2018170096. Epub 2018 Jun 15. Radiographics. 2018. PMID: 29906203 Review.
-
Evaluation of routine postoperative chest roentgenogram for determination of the correct position of permanent central venous catheters tip.J Res Med Sci. 2015 Jan;20(1):89-92. J Res Med Sci. 2015. PMID: 25767527 Free PMC article.
-
Cardiothoracic Medical Devices - A Pictorial Review.Semin Ultrasound CT MR. 2024 Dec;45(6):440-453. doi: 10.1053/j.sult.2024.07.008. Epub 2024 Jul 26. Semin Ultrasound CT MR. 2024. PMID: 39069276 Review.
Cited by
-
Who watches the WATCHMAN? A rare case of lower extremity paralysis.J Am Coll Emerg Physicians Open. 2023 Oct 7;4(5):e13052. doi: 10.1002/emp2.13052. eCollection 2023 Oct. J Am Coll Emerg Physicians Open. 2023. PMID: 37811359 Free PMC article.
-
Pre-deployment assessment of an AI model to assist radiologists in chest X-ray detection and identification of lead-less implanted electronic devices for pre-MRI safety screening: realized implementation needs and proposed operational solutions.J Med Imaging (Bellingham). 2022 Sep;9(5):054504. doi: 10.1117/1.JMI.9.5.054504. Epub 2022 Oct 26. J Med Imaging (Bellingham). 2022. PMID: 36310648 Free PMC article.
References
Publication types
LinkOut - more resources
Full Text Sources
Research Materials