

Trends in singleton preterm birth in Victoria, 2007 to 2017: A consecutive cross-sectional study
- PMID: 33382080
- PMCID: PMC8359202
- DOI: 10.1111/aogs.14074
Trends in singleton preterm birth in Victoria, 2007 to 2017: A consecutive cross-sectional study
Abstract
Introduction: Preterm birth is a major cause of perinatal morbidity and mortality worldwide. In many countries preterm birth rates are increasing, largely as a result of increases in iatrogenic preterm birth, whereas in other countries rates are stable or even declining. The objective of the study is to describe trends in singleton preterm births in Victoria from 2007 to 2017 in relation to trends in perinatal mortality to identify opportunities for improvements in clinical care.
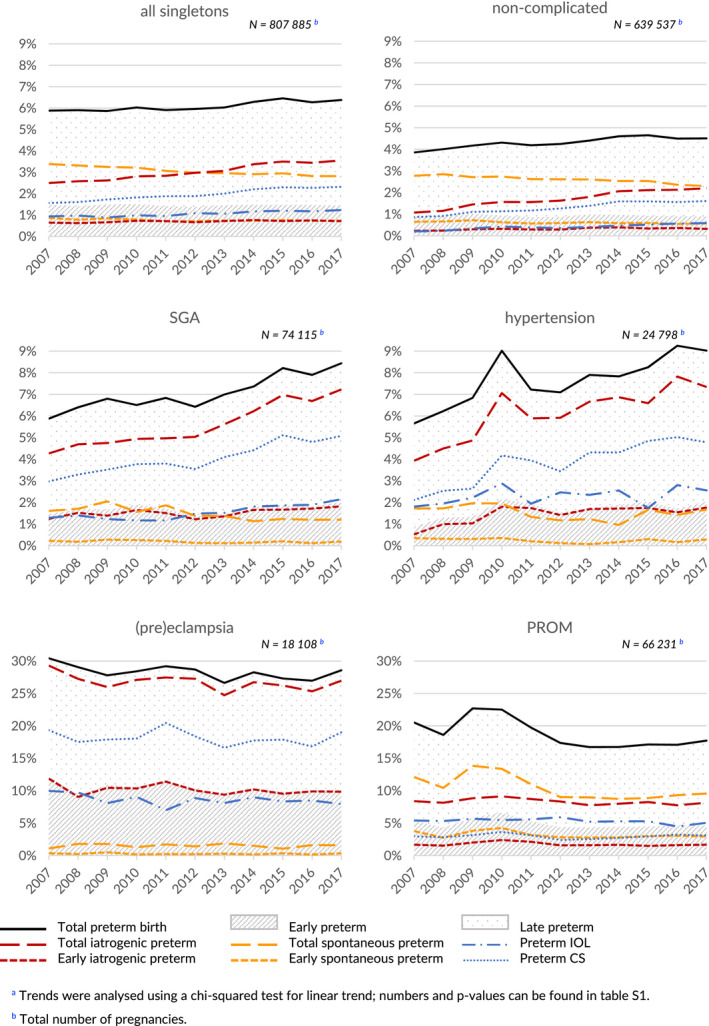
Material and methods: We conducted a consecutive cross-sectional study in all women with a singleton pregnancy giving birth at ≥20 weeks of pregnancy in Victoria, Australia, between 2007 and 2017, inclusive. Rates of preterm birth and perinatal mortality were calculated and trends were analyzed in all pregnancies, in pregnancies complicated by fetal growth problems, hypertension, (pre)eclampsia or prelabor rupture of membranes (PROM), and in (low-risk) pregnancies not complicated by any of these conditions.
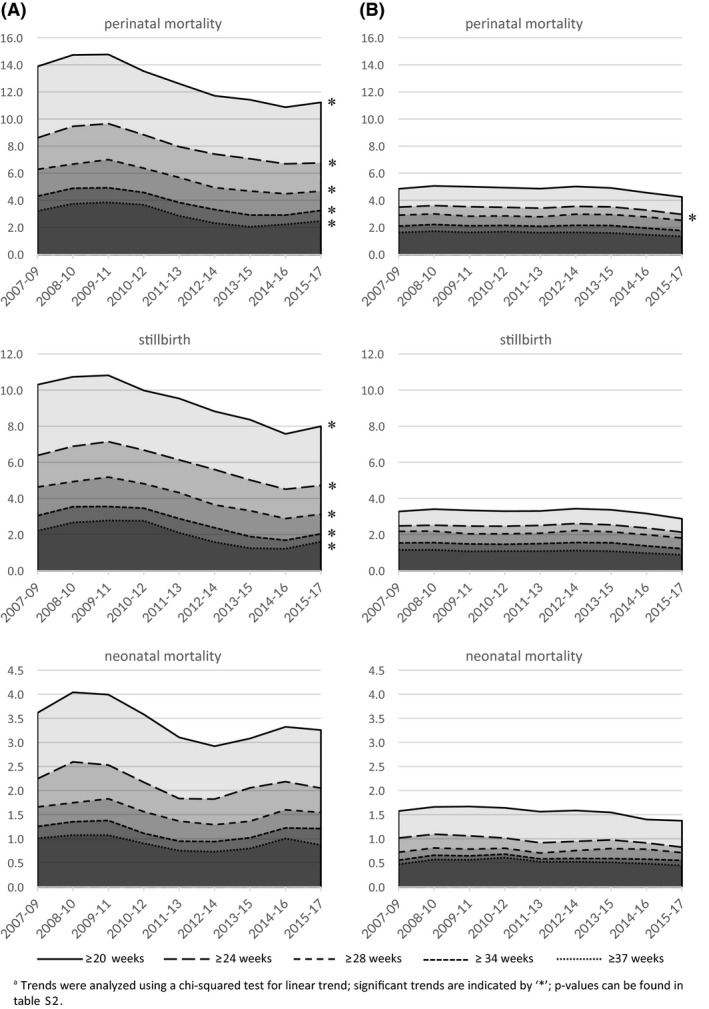
Results: There were 811 534 singleton births between 2007 and 2017. Preterm birth increased from 5.9% (4074 births) to 6.4% (4893 births; P < .001), due to an increase in iatrogenic preterm birth from 2.5% (1730 births) to 3.6% (2730 births; P < .001). Comparable trends were seen in pregnancies complicated by fetal growth problems and hypertension and in pregnancies not complicated by small for gestational age (SGA), hypertension, (pre)eclampsia or PROM (all P < .001). In pregnancies complicated by SGA, hypertension, (pre)eclampsia or PROM the perinatal mortality rate from 20 weeks of gestation fell (13 to 12 per 1000 births; P < .001). In pregnancies not complicated by SGA, hypertension, (pre)eclampsia or PROM there was no significant change in the perinatal mortality from 28 weeks and no decrease in the preterm weekly prospective stillbirth risk.
Conclusions: The singleton preterm birth rate in Victoria is increasing, driven by an increase in iatrogenic preterm birth, both in pregnancies complicated by SGA and hypertension, and in pregnancies not complicated by SGA, hypertension, (pre)eclampsia or PROM. While perinatal mortality decreased in the pregnancies complicated by SGA, hypertension, (pre)eclampsia or PROM, no significant reduction in perinatal mortality from 28 weeks or in preterm weekly prospective stillbirth risk was noted in the pregnancies not complicated by any of these conditions.
Keywords: hypertensive disorders in pregnancy; iatrogenic preterm birth; induction of labor; perinatal morbidity and mortality; preterm birth; preterm prelabor rupture of membranes; small for gestational age; spontaneous preterm birth.
© 2020 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
BWM reports consultancy for ObsEva, Merck and Guerbet. MAD is a part‐time employee of the Consultative Councils Unit, which manages the Victorian Perinatal Data Collection. EMW is the CEO of Safer Care Victoria. All other authors report no conflict of interest.
Figures

References
-
- Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379:2162‐2172. - PubMed
-
- Woythaler MA, McCormick MC, Smith VC. Late preterm infants have worse 24‐month neurodevelopmental outcomes than term infants. Pediatrics. 2011;127:e622‐e629. - PubMed
-
- Zwertbroek EF, Franssen MTM, Broekhuijsen K, et al. Neonatal developmental and behavioral outcomes of immediate delivery versus expectant monitoring in mild hypertensive disorders of pregnancy: 2‐year outcomes of the HYPITAT‐II trial. Am J Obstet Gynecol. 2019;221:154.e1‐154.e11. - PubMed
-
- Saigal S, Doyle LW. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet. 2008;371:261‐269. - PubMed
-
- Kugelman A, Colin AA. Late preterm infants: near term but still in a critical developmental time period. Pediatrics. 2013;132:741‐751. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
